[vc_row type=”full_width_content” full_screen_row_position=”middle” equal_height=”yes” content_placement=”middle” bg_color=”#ffffff” scene_position=”center” text_color=”light” text_align=”left” overlay_strength=”0.3″ shape_divider_position=”bottom” bg_image_animation=”none”][vc_column column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_link_target=”_self” column_shadow=”none” column_border_radius=”none” width=”1/1″ tablet_width_inherit=”default” tablet_text_alignment=”center” phone_text_alignment=”center” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”]
Multiple Sclerosis (MS)
[/vc_column_text][/vc_column_inner][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/3″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none” alignment=”right”][mpc_button preset=”mpc_preset_26″ url=”url:%23modal_id_reviewers|||” font_preset=”default” font_color=”#ffffff” font_size=”13″ font_line_height=”1.3″ font_transform=”uppercase” font_align=”right” title=”Reviewers” icon_size=”14″ background_color=”#555555″ border_css=”border-width:0px;border-color:#444444;border-style:solid;border-radius:3px;” padding_divider=”true” padding_css=”padding-top:8px;padding-right:8px;padding-bottom:8px;padding-left:8px;” margin_divider=”true” margin_css=”margin-top:10px;margin-right:2px;” hover_background_color=”#333333″ hover_border_css=”border-color:#444444;border-style:solid;”][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”none” text_align=”left” css=”.vc_custom_1565287910523{margin-top: -20px !important;}”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][mpc_button preset=”mpc_preset_26″ url=”url:%23modal_id_5ced944b48d3f|||” font_preset=”default” font_color=”#ffffff” font_size=”13″ font_line_height=”1.3″ font_transform=”uppercase” title=”Quick Review” icon_size=”14″ background_color=”#555555″ border_css=”border-width:0px;border-color:#444444;border-style:solid;border-radius:3px;” padding_divider=”true” padding_css=”padding-top:8px;padding-right:8px;padding-bottom:8px;padding-left:8px;” margin_divider=”true” margin_css=”margin-top:10px;margin-right:2px;” hover_background_color=”#333333″ hover_border_css=”border-color:#444444;border-style:solid;”][mpc_button preset=”mpc_preset_26″ url=”url:%23modal_id_brochure|||” font_preset=”default” font_color=”#ffffff” font_size=”13″ font_line_height=”1.3″ font_transform=”uppercase” title=”Patient Brochure” icon_size=”14″ background_color=”#555555″ border_css=”border-width:0px;border-color:#444444;border-style:solid;border-radius:3px;” padding_divider=”true” padding_css=”padding-top:8px;padding-right:8px;padding-bottom:8px;padding-left:8px;” margin_divider=”true” margin_css=”margin-top:10px;margin-right:2px;” hover_background_color=”#333333″ hover_border_css=”border-color:#444444;border-style:solid;”][/vc_column_inner][/vc_row_inner][mpc_modal preset=”mpc_preset_5″ frequency=”onclick” onclick_id=”modal_id_5ced944b48d3f” max_width=”75″ max_height=”75″ position=”bottom-center” close_overlay=”true” mpc_icon__transition=”fade” mpc_icon__icon=”eti eti_close” mpc_icon__icon_color=”#555555″ mpc_icon__icon_size=”24″ mpc_icon__background_color=”#f3f3f3″ mpc_icon__border_css=”border-width:1px;border-color:#f3f3f3;border-style:solid;border-radius:99px;” mpc_icon__padding_css=”padding:10px;” mpc_icon__margin_divider=”true” mpc_icon__margin_css=”margin-top:-40px;margin-right:-40px;” mpc_icon__hover_icon_color=”#333333″ mpc_icon__hover_background_color=”#e5e5e5″ mpc_icon__hover_border_css=”border-width:5px;border-color:#e5e5e5;border-style:solid;border-radius:99px;” overlay_background_color=”rgba(48,48,48,0.48)” background_color=”#f7f7f7″ border_css=”border-width:15px;border-color:#e5e5e5;border-style:solid;” padding_css=”padding:40px;” animation_in_type=”transition.slideDownBigIn” animation_in_offset=”100″ animation_in_duration=”1200″ animation_in_delay=”1000″][vc_column_text]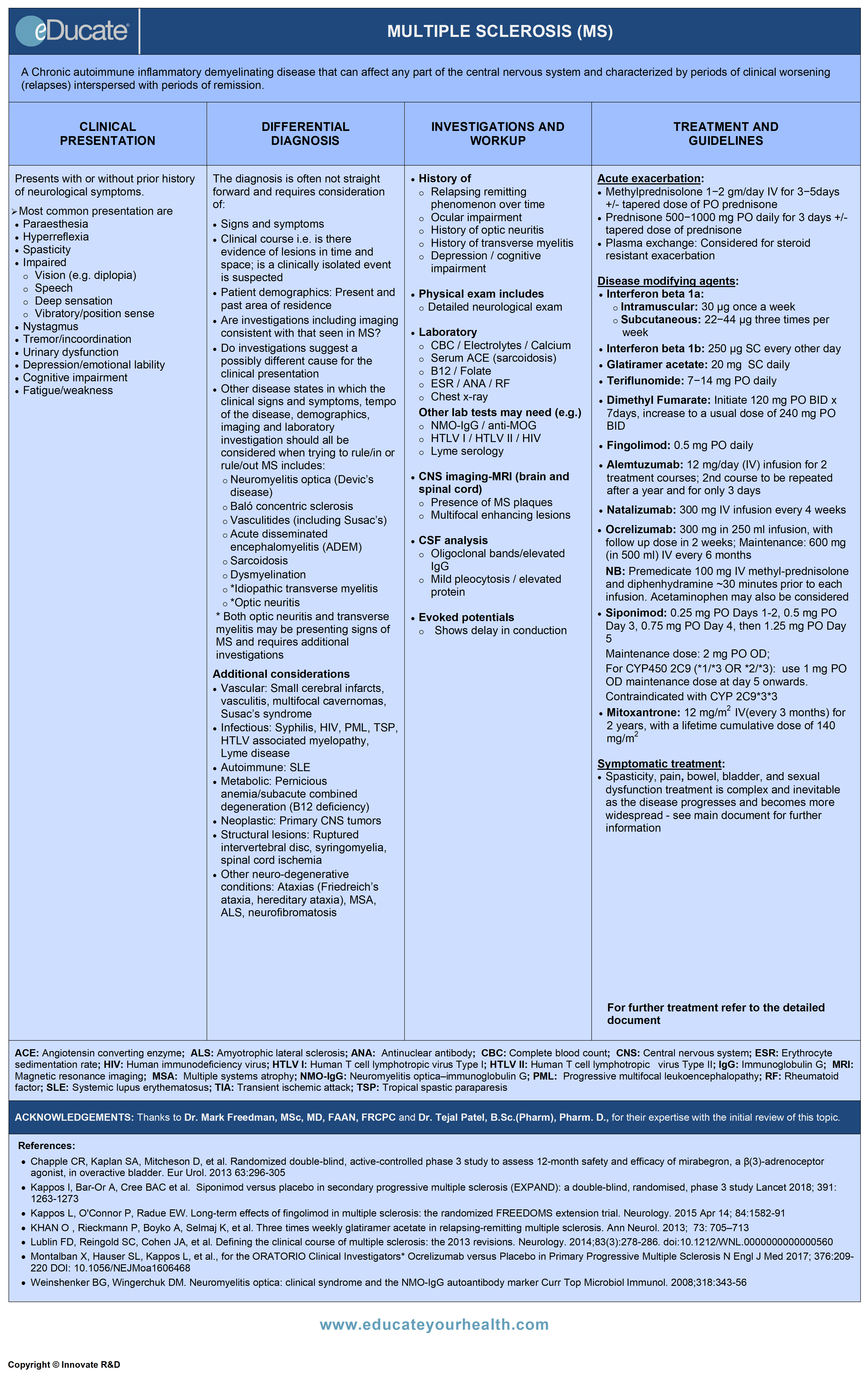 [/vc_column_text][/mpc_modal][mpc_modal preset=”mpc_preset_5″ frequency=”onclick” onclick_id=”modal_id_reviewers” max_width=”40″ max_height=”40″ mpc_icon__transition=”fade” mpc_icon__icon=”eti eti_close” mpc_icon__icon_color=”#555555″ mpc_icon__icon_size=”24″ mpc_icon__background_color=”#f3f3f3″ mpc_icon__border_css=”border-width:1px;border-color:#f3f3f3;border-style:solid;border-radius:99px;” mpc_icon__padding_css=”padding:10px;” mpc_icon__margin_divider=”true” mpc_icon__margin_css=”margin-top:-40px;margin-right:-40px;” mpc_icon__hover_icon_color=”#333333″ mpc_icon__hover_background_color=”#e5e5e5″ mpc_icon__hover_border_css=”border-width:5px;border-color:#e5e5e5;border-style:solid;border-radius:99px;” overlay_background_color=”rgba(48,48,48,0.48)” background_color=”#f7f7f7″ border_css=”border-width:15px;border-color:#e5e5e5;border-style:solid;” padding_css=”padding:40px;” animation_in_type=”transition.slideDownBigIn” animation_in_offset=”100″ animation_in_duration=”1200″ animation_in_delay=”1000″][vc_column_text]ACKNOWLEDGEMENTS:
[/vc_column_text][/mpc_modal][mpc_modal preset=”mpc_preset_5″ frequency=”onclick” onclick_id=”modal_id_reviewers” max_width=”40″ max_height=”40″ mpc_icon__transition=”fade” mpc_icon__icon=”eti eti_close” mpc_icon__icon_color=”#555555″ mpc_icon__icon_size=”24″ mpc_icon__background_color=”#f3f3f3″ mpc_icon__border_css=”border-width:1px;border-color:#f3f3f3;border-style:solid;border-radius:99px;” mpc_icon__padding_css=”padding:10px;” mpc_icon__margin_divider=”true” mpc_icon__margin_css=”margin-top:-40px;margin-right:-40px;” mpc_icon__hover_icon_color=”#333333″ mpc_icon__hover_background_color=”#e5e5e5″ mpc_icon__hover_border_css=”border-width:5px;border-color:#e5e5e5;border-style:solid;border-radius:99px;” overlay_background_color=”rgba(48,48,48,0.48)” background_color=”#f7f7f7″ border_css=”border-width:15px;border-color:#e5e5e5;border-style:solid;” padding_css=”padding:40px;” animation_in_type=”transition.slideDownBigIn” animation_in_offset=”100″ animation_in_duration=”1200″ animation_in_delay=”1000″][vc_column_text]ACKNOWLEDGEMENTS:
Thanks to Dr. Mark Freedman, MSc, MD, FAAN, FRCPC, Professor of Medicine (Neurology), University of Ottawa, Director, Multiple Sclerosis Research Unit, The Ottawa Hospital-General Campus, Ottawa, ON Canada, and Dr. Tejal Patel, B.Sc.(Pharm), Pharm. D., Clinical Assistant Professor, School of Pharmacy, University of Waterloo, ON Canada for their expertise with the initial review of this topic.[/vc_column_text][/mpc_modal][mpc_modal preset=”mpc_preset_5″ frequency=”onclick” onclick_id=”modal_id_brochure” max_width=”75″ max_height=”75″ position=”bottom-center” close_overlay=”true” mpc_icon__transition=”fade” mpc_icon__icon=”eti eti_close” mpc_icon__icon_color=”#555555″ mpc_icon__icon_size=”24″ mpc_icon__background_color=”#f3f3f3″ mpc_icon__border_css=”border-width:1px;border-color:#f3f3f3;border-style:solid;border-radius:99px;” mpc_icon__padding_css=”padding:10px;” mpc_icon__margin_divider=”true” mpc_icon__margin_css=”margin-top:-40px;margin-right:-40px;” mpc_icon__hover_icon_color=”#333333″ mpc_icon__hover_background_color=”#e5e5e5″ mpc_icon__hover_border_css=”border-width:5px;border-color:#e5e5e5;border-style:solid;border-radius:99px;” overlay_background_color=”rgba(48,48,48,0.48)” background_color=”#f7f7f7″ border_css=”border-width:15px;border-color:#e5e5e5;border-style:solid;” padding_css=”padding:40px;” animation_in_type=”transition.slideDownBigIn” animation_in_offset=”100″ animation_in_duration=”1200″ animation_in_delay=”1000″][vc_column_text][pdf-embedder url=”https://www.educateyourhealth.com/wp-content/uploads/2019/04/Multiple-Sclerosis-Brochure.pdf” width=”750″][/vc_column_text][/mpc_modal][mpc_modal preset=”mpc_preset_5″ frequency=”onclick” onclick_id=”modal_id_video” max_width=”65″ max_height=”85″ mpc_icon__transition=”fade” mpc_icon__icon=”eti eti_close” mpc_icon__icon_color=”#555555″ mpc_icon__icon_size=”24″ mpc_icon__background_color=”#f3f3f3″ mpc_icon__border_css=”border-width:1px;border-color:#f3f3f3;border-style:solid;border-radius:99px;” mpc_icon__padding_css=”padding:10px;” mpc_icon__margin_divider=”true” mpc_icon__margin_css=”margin-top:-40px;margin-right:-40px;” mpc_icon__hover_icon_color=”#333333″ mpc_icon__hover_background_color=”#e5e5e5″ mpc_icon__hover_border_css=”border-width:5px;border-color:#e5e5e5;border-style:solid;border-radius:99px;” overlay_background_color=”rgba(48,48,48,0.48)” background_color=”#f7f7f7″ border_css=”border-width:15px;border-color:#e5e5e5;border-style:solid;” padding_css=”padding:40px;” animation_in_type=”transition.slideDownBigIn” animation_in_offset=”100″ animation_in_duration=”1200″ animation_in_delay=”1000″][vc_column_text]
[/vc_column_text][/mpc_modal][divider line_type=”Full Width Line” line_thickness=”1″ divider_color=”default” custom_height=”30″][/vc_column][/vc_row][vc_row type=”in_container” full_screen_row_position=”middle” scene_position=”center” text_color=”dark” text_align=”left” top_padding=”10″ class=”zindexbottom elementup” overlay_strength=”0.3″ shape_divider_position=”bottom” bg_image_animation=”none” shape_type=””][vc_column column_padding=”no-extra-padding” column_padding_position=”all” background_color=”#fcfcfc” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_link_target=”_self” column_shadow=”none” column_border_radius=”none” width=”1/1″ tablet_width_inherit=”default” tablet_text_alignment=”default” phone_text_alignment=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_row_inner column_margin=”default” text_align=”left” el_id=”definition-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Definition
[/vc_column_text][vc_column_text]A Chronic autoimmune inflammatory demyelinating disease that can affect any part of the central nervous system and characterized by periods of clinical worsening (relapses) interspersed with periods of remission.[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”etiology-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Etiology
[/vc_column_text][vc_column_text]Unknown, but appears to be a compilation of several factors which include: genetic susceptibility, viral or environmental factors, and autoimmune dysfunction.
- Genetic susceptibility/predisposition
- HLA linkage through HLA-DR2 and alleles of interleukin 2 (IL-2) and 7 (IL-7) receptor alpha gene
- Other “hot spots” include genes for IL-7 and IL-20
- Genetic predisposition is also suggested by increased risk in some ethnic groups (e.g., Caucasians of northern European ancestry) and decreased risk in others (e.g., Native Americans)
- Interestingly, 70% of identical twins are discordant for MS, implicating environmental and other unknown factors in MS susceptibility
- Environmental factors:
- Latitudinal gradient in the MS prevalence, which increases further from the equator in both hemispheres
- Migration studies have observed that individuals who move from one area to another before the age of 15 years acquire the MS prevalence rate of the new region
- Vitamin D deficiency, possibly secondary to reduced sun exposure
- Cigarette smoking
- Obesity
- Viral etiology:
- Epstein bar virus(EBV) continues to be of interest, particularly in pediatric studies; The frequency of MS is low in those who are seronegative for EBV, but increased in those history of infectious mononucleosis
- Autoimmune dysfunction
- Pathological lymphocytic infiltrates in acute plaques
- Changes in peripheral blood lymphocytes similar to autoimmune patterns in animal models
- Improvement or remission with drugs modulating or suppressing the immune system
Classification:
The diagnosis of MS is made on clinical grounds with input from imaging and other laboratory studies. There are four main subtypes and other observed syndromes as follows:
- Relapsing-remitting MS (RRMS)
- Most common initial presentation in 85-90% of patients
- Periods of relapse during which time new symptoms can appear, followed by periods of stability, irrespective of whether the recovery is complete or incomplete
- Secondary progressive MS (SPMS)
- Evolves from RRMS
- SPMS is often typically preceded by a variable period (2–40 years) of RRMS
- Steady progression of clinical neurologic damage in the absence of intervening relapses
- Relapses, often with residual deficits may or may not ensue
- Primary progressive MS (PPMS)
- Represents 10-15% of those with MS
- Gradual progression with a changing slope
- No apparent relapses
- Progressive relapsing MS (PRMS)
- Least common form of MS
- Steady cumulative progression of clinical neurologic damage
- Superimposed relapses with or without remissions
- Other:
- Clinically Isolated Syndrome (CIS): The first clinical presentation of a disease that shows characteristics of inflammatory demyelination that could be MS, but has yet to fulfill criteria of dissemination in time
- Radiologically Isolated Syndrome (RIS): Incidental imaging suggests inflammatory demyelination in the absence of clinical signs or symptoms. Not considered an MS subtype, as clinical evidence lacking
[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”epidemiology-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Epidemiology
[/vc_column_text][vc_column_text]The leading cause of nontraumatic neurologic disability in the young.
- Typical age of onset: 20-40 years; range: 2-80 years
- Mean age of onset 32 years
- Female > Male
- Worldwide incidence ~0.1%
- Prevalence
- Canada ~55,00 0- 100,000
- USA ~350,000 – 400,000
- Worldwide ~2.5 million
- Increased incidence observed when moving away from the equator in either direction
- Economic impact: Cost of managing disease plus disability plus loss of manpower productivity for patient and caregivers (the greatest cause of acquired non-traumatic neurological impairment in young people)
- Death often results from medical complications (e.g. infections)
[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”pathophysiology-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Pathophysiology
[/vc_column_text][vc_column_text]
- Demyelination: An immune-mediated inflammation which denudes axons of their myelin sheath
- Demyelination is often followed by attempts of remyelination
- The cycle of demyelination and remyelination, leads to inadequate and often ineffective myelination
- Axonal injury occurs as either “collateral” damage to the inflammation or as a part of the disease process
- The initial relapsing-remitting process may evolve into a secondary progression
The mechanism is as follows:
 [/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”clinical-presentation-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”clinical-presentation-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Clinical Presentation
[/vc_column_text][vc_column_text]Variable neurological symptoms separated in space (depending on CNS areas involved) and time by months or years. There may well be a threshold beyond which progressive neurological decline may ensue.
Common eventual signs and symptoms are:
- Fatigue and generalized weakness
- Vision disturbances: Impaired or double vision, nystagmus
- Motor dysfunction: Focal weakness, tremor, incoordination, paroxysmal muscle spasms
- Sensory disturbances: Paraesthesias, impaired deep sensation, impaired vibratory and position sense
- Impaired speech: Slurring, scanning (dysarthria)
- Abnormal reflexes: Absent or exaggerated
- Urinary dysfunction:
- Hesitancy, frequency, urgency, retention, incontinence; urinary tract infections (UTI)
- Urinary dysfunction affects about 90% of patients with MS and UTIs may exacerbate relapse of MS
- Neurobehavioral syndromes: Depression, cognitive impairment, emotional lability
Symptoms of MS are often unpredictable, varying from person to person and from time to time in the same person.[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”differential-diagnosis-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Differential Diagnosis
[/vc_column_text][vc_column_text]The diagnosis leading to MS is often not straightforward and requires consideration of:
- Signs and symptoms
- Clinical course i.e. there is evidence of lesions in time and space
- Patient demographics
- Investigations including imaging are consistent with that seen in MS
- A possible different cause for the clinical presentation
- Other disease states considered to rule out a diagnosis of MS includes:
- NMO Spectrum Disorder (Devic’s disease)
- Anti-MOG (Myelin oligodendrocyte glycoprotein) antibody syndrome
- Baló’s concentric sclerosis (rare diagnosis)
- Vasculitides (including Susac’s syndrome)
- Acute disseminated encephalomyelitis (ADEM)
- Sarcoidosis
- Dysmyelination (leukodystrophy)
- Idiopathic transverse myelitis*
- Optic neuritis*
* Both optic neuritis and transverse myelitis may be presenting signs of MS and requires additional investigations, however, the progression to MS is not absolute, in that ~60-90% of those with abnormal brain MRI lesions may develop MS while there is ~20% of MS in those whose brain MRI is initially normal.
Additional considerations:
- Vascular: Small cerebral infarcts, vasculitis, multifocal cavernomas, Susac’s syndrome
- Infectious: Syphilis, HIV, progressive multifocal leukoencephalopathy (PML), tropical spastic paraparesis (TSP), HTLV associated myelopathy, Lyme disease
- Autoimmune: Systemic lupus erythematosus (SLE), Behcet’s disease
- Metabolic: Pernicious anemia/subacute combined degeneration (B12 deficiency)
- Neoplastic: Primary CNS tumors
- Structural lesions: Ruptured intervertebral disc, syringomyelia, spinal cord ischemia
- Other neuro-degenerative conditions: Ataxias (Friedreich’s ataxia, hereditary ataxia), multiple systems atrophy (MSA), amyotrophic lateral sclerosis (ALS), neurofibromatosis
- Drug-induced demyelination with antitumor necrosis factor therapies for other inflammatory conditions such as Crohn disease or rheumatoid or psoriatic arthritis
Ref: Miller DH et al. MultScler, 2008; 14:1157-74 for a consensus approach on the differential diagnosis of suspected MS including diagnostic pathways.[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”investigation-and-workup-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Investigation and Workup
[/vc_column_text][vc_column_text]History:
- History of previous transient neurological episodes, including duration of events and recurrence
- Information of relapsing-remitting phenomenon over time
- Ocular history – including acuity, loss of color vision
- History of depression or cognitive impairment
Other symptoms:
Bowel/bladder
- Urinary urgency and frequency may progress to incontinence and bladder atony
- Urinary tract infections are common in MS (F > M), further contributes to bladder dysfunction
- Constipation, fecal incontinence
Pain
- Common complaint
- Approximately 43% of patients report one or more painful symptoms such as trigeminal neuralgia, Lhermitte’s phenomenon, dysesthesia, back pain, visceral pain, and pain due to muscle spasms
Sexual dysfunction
- Men experience various degrees of erectile dysfunction
- Women may experience a lack of sensitivity and dyspareunia due to decreased vaginal lubrication
Uhthoff’s phenomenon
- Exposure to hot conditions (sun, sauna, hot-tubs, etc.) transiently worsens neurological symptoms
- Mechanism likely related to conduction block
Fatigue
- The degree of fatigue is discordant with the level of activity. May precede focal neurological symptoms
Depression
- More than 50% of patients may have some degree of depression
- Multifactorial, related to psychological aspect of acquiring a potentially debilitating chronic progressive disorder ±co-morbidities
Cognitive dysfunction
- Cognitive impairment occurs in 34-65% of patients
- Maybe present at the time of detection of MS
Epilepsy
- 2-3% of patients may develop epilepsy
Neurological Examination
Optic nerve assessment for optic neuritis (ON)
Symptoms:
- Recent visual disturbances, pain in the eye exacerbated on movement
- Variable degree of visual loss (scotoma) affecting mainly central vision
- Seldom involves both eyes
Signs:
- A moving flashlight produces an unequal pupillary constriction, due to an afferent pupillary defect (Marcus Gunn pupil) on the affected side
- Optic disc edema is a rare finding and would suggest something else
- In retrobulbar lesions; initially, fundus may appear normal, however; pallor may ensue later as a result of axonal loss and gliosis
- Approximately 90% of patients regain normal vision over 2-6 months
Internuclear ophthalmoplegia
- Abnormal horizontal ocular movements with lost or delayed adduction
- Horizontal nystagmus of the abducting eye
- Lesion of the medial longitudinal fasciculus on the side of diminished adduction
- Convergence preserved
Nystagmus
- Horizontal, rotational and vertical nystagmus can all be seen with lesions involving various parts of the brain stem and/or cerebellum
- Pendular nystagmus (rapid, small-amplitude pendular oscillations of the eyes) can be present in <4% of MS patients
Vertigo
Symptoms
- Sense of movement (often rotational) of a person or to an external environment. Maybe due to brain stem plaques
- May also occur in conjunction with other brainstem findings including nystagmus, diplopia, facial weakness or dysesthesia, hyper- or hypoacusis, and long tract signs (hemi-sensory or hemi-motor deficits)
Signs:
- Positive Dix-Hallpike maneuver: Up or down beating, non-rotational nystagmus, without latency (patient lying with neck extended off the examining table and head angled to left or right)
Sensory disturbance:
Symptoms
- Numbness, tingling, pins-and-needles
- Band-like tightness around limbs or torso
- Decreased sensitivity to light touch
- Paraesthesia, impaired deep, vibratory and positional sensations
Signs
Variable and related to sensory pathway involved
- Impairment of pinprick and temperature if spinothalamic tract affected
- Impairment of vibration and light touch, joint position sense if posterior column involved
- Patchy areas of reduced pain and perception in the limbs and trunk
Lhermitte’s phenomenon
- Transient sensory disturbance with the sensation of an electric-like shock radiating down the spine into the limbs triggered by neck flexion
- Occurs with other lesions of the upper cervical cord including tumors, cervical disc herniation, and trauma
Motor symptoms
Symptoms
- Face, limb or trunk weakness ± associated in-coordination
Signs (typically related to upper motor neuron findings)
- Limb paresis progressing to plegia
- Often asymmetric, can lead to hemiparesis/plegia or paraparesis/plegia or tetraparesis/plegia
- Increased tone/spasticity
- Hyperreflexia – including clonus, spread of reflexes i.e. activating one reflex recruit another reflex pathway, Babinski sign (extensor plantar response)
- Hyporeflexia – may reflect hypotonia resulting from cerebellar involvement
- Unilateral facial paresis – both upper motor neuron (Bell’s palsy) and lower motor neuron facial weakness can occur
- Limb amyotrophy as well as facial myokymia (fine undulating wave-like facial twitching
- Hemifacial spasm can be associated with MS
Coordination and balance
Symptoms
- Incoordination of limbs (including finger dexterity), trunk and gait
- Impact on ADLs such as writing, eating, dressing, walking, etc.
Signs (typically related to cerebellar findings)
- Nystagmus
- Speech disturbance (staccato or scanning or telegraphic speech)
- Dysarthria and dysphagia
- Limb dysmetria/ataxia – uni or bilateral
- Gait and truncal ataxia with tendency to falls
- Astasia (inability to stand)
- Hypotonia (decreased tone)
- Intention tremor
Cognitive dysfunction
Symptoms
- Cognitive decline may be discordant with clinical exacerbations
- Manifests in poor memory and information processing, inattention and difficulty with abstract thought
Signs
- Poor performance on standardized tests
- Mini-mental status exam (MMSE)
- Montreal cognitive assessment (MoCA)
Laboratory
Blood
- Complete blood count (CBC)
- Electrolytes, calcium
- B12, folate
- Erythrocyte sedimentation rate (ESR)
- ANA/rheumatoid factor
- Antiphospholipid/anticardiolipin antibodies
- Thyroid studies (freeT4, TSH)
- NMO-IgG [if neuromyelitis optica suspected]
- Anti-MOG antibodies
- Lyme serology (if in an endemic area)
- Serology for HTLV I/HTLV II (if tropical spastic paraparesis suspected)
- HIV (if suspected)
CNS Imaging
MRI
- 95% sensitive in patients with established disease
- Detects white matter lesions within the brain and spinal cord
- T2 weighted images:
- Hyperintensities lesions typically periventricular and corpus callosum
- However, Juxtacortical lesions have been reported
- Provide information about disease burden
- T1 weighted images:
- Hypointense black holes suggest areas of permanent axonal/tissue injury/gliosis
- Gadolinium infusion enhances lesions on T1 images and indicates active inflammation; ring-enhancing mass-like lesions may be suggestive of tumefactive MS
- Lesions may enhance for up 4-6 weeks post-exacerbation; only 3–5% of MS lesions enhance for >8 weeks, hence persistent enhancement may suggest other pathology, e.g. neurosarcoidosis
- MRI showing multifocal enhancing lesions with first clinical presentation raises the possibility of MS vs. other disseminated diseases such as acute disseminated encephalomyelitis (ADEM) or neoplasm, sarcoidosis, progressive multifocal leukoencephalopathy (PML)
2010 McDonald criteria for the diagnosis of multiple sclerosis
{kind=link}
The revised McDonald criteria replaced the previously used terms such as “clinically definite” and “probable MS” with the following:
- The diagnosis of “MS” is given if diagnostic criteria are fulfilled
- The diagnosis of “possible MS” is given if the criteria are not completely met
- The diagnosis of “not MS” is given if the criteria are fully explored and not met
CSF analysis
- Oligoclonal bands: Distinct electrophoretic patterns reflecting elevation of IgG, present in >95% of patients with established disease but can be non-specific, as the MRI, and may be seen in other neurodegenerative conditions and CNS infections
- Elevated IgG index in <90% of patients (values reported as >0.7)
- Mild pleocytosis (unusual to have WBC >50)
- Mildly elevated protein is not unusual
Evoked Potentials
- A measure of electrical conductance along the neuroaxis
- Electrodes placed at different points over peripheral nerves, spinal cord and cortex can be used to detect conduction delays in an induced electrical potential
- Delays in conduction may help to localize lesions
- Types of evoked potentials:
- Somatosensory evoked potential (SSEP)
- Brainstem auditory evoked potential (BAER)
- Motor evoked potentials via magnetic stimulation
- Visual evoked potentials (VEP)-(the most useful of all)
[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”treatment-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Treatment
[/vc_column_text][cq_vc_tabs tabsstyle=”style2″ titlebg=”#16847d” titlehoverbg=”#333333″ rotatetabs=”0″][cq_vc_tab_item tabtitle=”Management & Therapies”]Goal is to:
- Shorten the acute exacerbation
- Decrease the frequency of acute attacks and delay disease progression
- Relieve the symptoms to maintain the quality of life
Treatment strategies:
- a) Treatment of acute exacerbation
- b) Disease-modifying therapy
- c) Symptomatic treatment
- d) Non-pharmacological treatment
A) Acute exacerbations:
For patients presenting with functional impairment, in acute phase, the recommended first-line treatment is glucocorticoids.
- Methylprednisolone: 1 g/day IV usually for 3-5 days (but can be used up to 10 days). Maybe followed by a tapering dose of oral prednisone (e.g. 100 mg x 1 dose then decrease by 10 mg daily until finished)
- Prednisone: 500-1000 mg PO daily for 3-5 days. Maybe followed by a tapering dose of oral prednisone
- Plasma exchange: Considered for steroid-resistant exacerbation
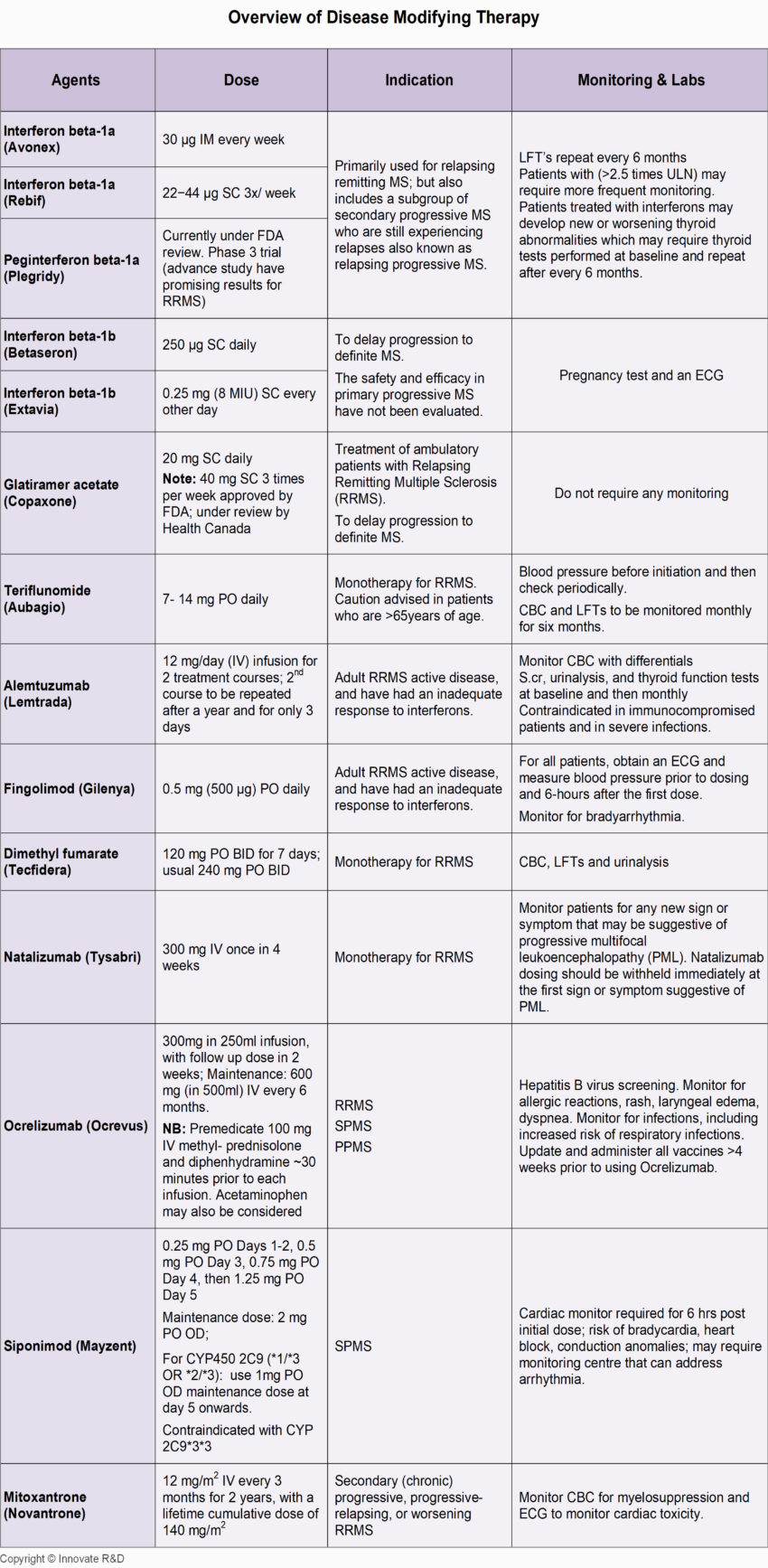
B) Disease-modifying therapy:
Indications:
- Relapsing-remitting (RRMS) phase
- Secondary progressive multiple sclerosis (SPMS)
- Primary progressive (PPMS)
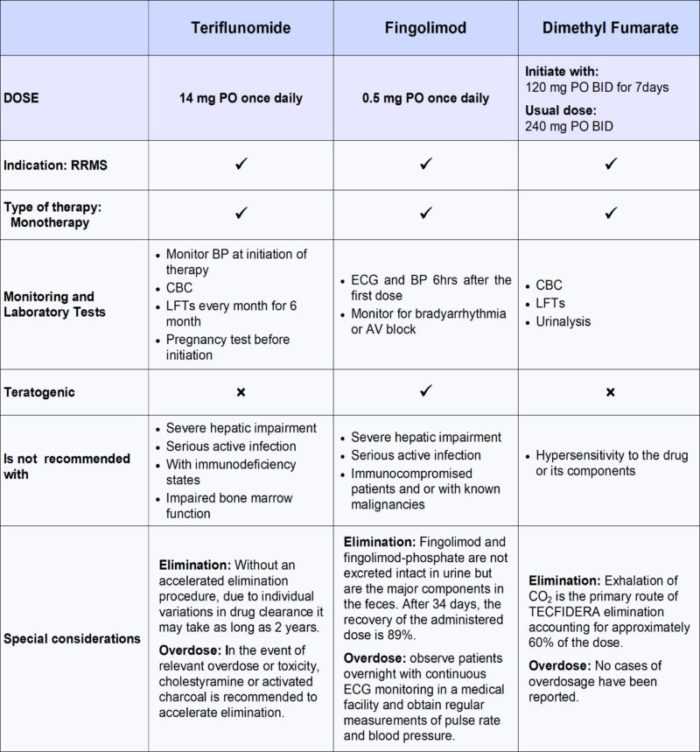
Comparison of Oral Disease-Modifying Therapies in MS
Other agents which have been tried but without proven benefit include:
Cyclophosphamide:
- Dose: 700 mg/m2 IV; every month along with 1 g of methylprednisolone
- Highly myelosuppressive; monitor absolute neutrophils count for dose adjustment
Other experimental modalities include:
- Hematopoietic stem cell transplantation
Intravenous immunoglobulin (IVIG):
- In the partum or immediate post-partum period
- Induction with 0.4 g/kg daily for 5 days followed by monthly 1 g/kg
C) Symptomatic treatment:
- Inevitable as disease advances
- Complex due to the widespread compromise of CNS function
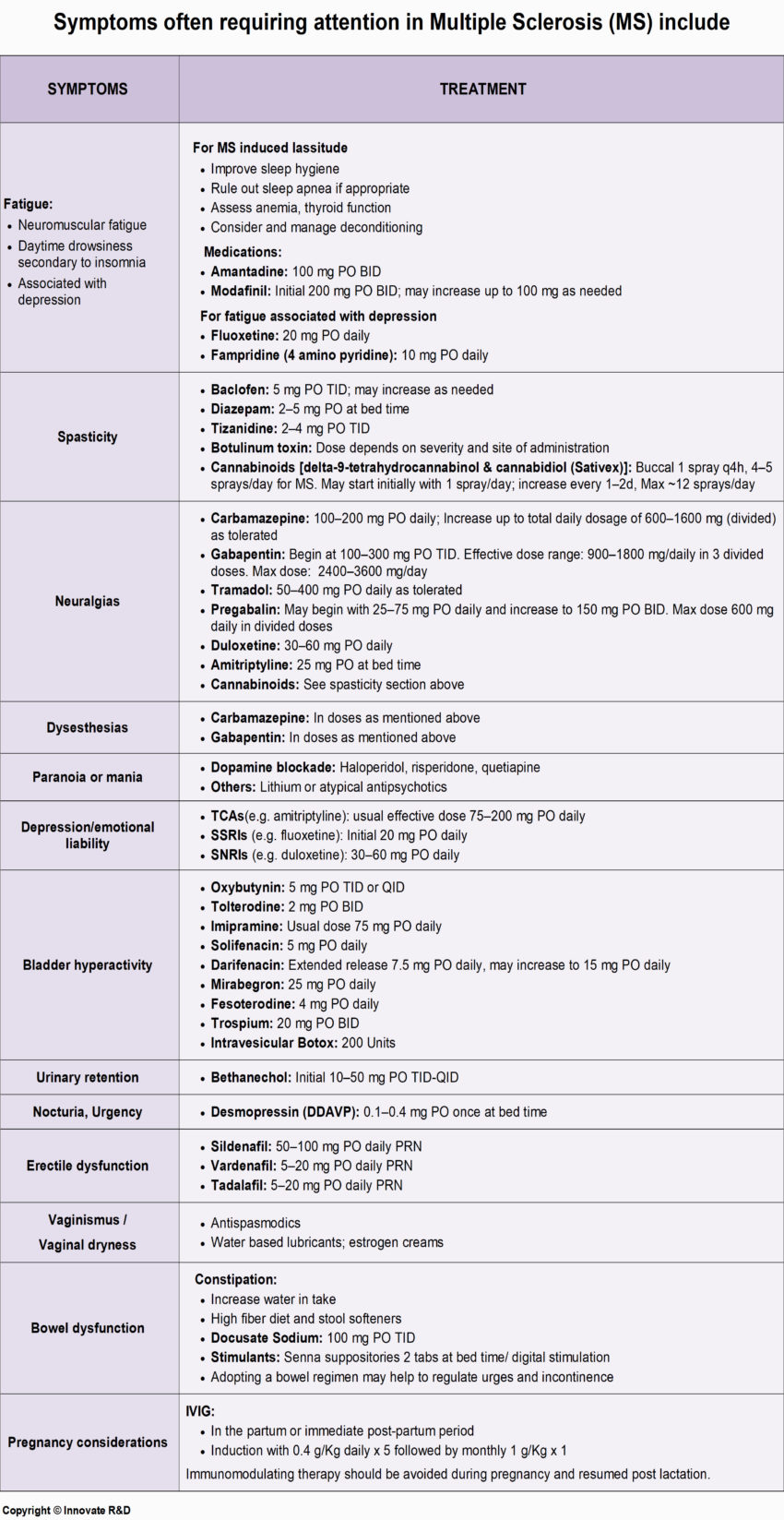 1) Spasticity:
1) Spasticity:
Pain and constipation may trigger spasticity. Assess and treat before using antispasmodics.
Treatment:
Baclofen:
- Dose: 5-10 mg PO TID
- Maximum dose: 80 mg/day
Tizanidine:
- Dose: 2-4 mg PO TID
- Maximum dose: 36 mg/day
Gabapentin:
- Dose: Begin at 100 to 300 mg TID
- Effective dose range: 900-1800 mg/daily in 3 divided doses
- Maximum dose: 2400 mg-3600 mg/day
Diazepam:
- Dose: 5-10 mg PO TID PRN
Cannabinoids (delta-9-tetrahydrocannabinol & cannabidiol)
- Dose: Buccal 1 spray every 4 hr, 4-5 sprays/day for MS
- May start initially with 1 spray/day; increase every 1-2 days; Max. ~12 sprays/day
Caution: Abrupt discontinuation of the above agents may cause seizures and withdrawal symptoms.
Botulinum toxin:
- Dose-dependent on site of administration and severity of the disease
2) Fatigue:
May be characterized as:
- Neuromuscular fatigue
- Daytime drowsiness secondary to insomnia
- Fatigue associated with depression
Treatment:
Amantadine:
- Dose: 100 mg PO BID; may improve MS associated lassitude
Modafinil:
- Dose: 100 mg PO BID
Antidepressant:
- For fatigue associated with depression(e.g. fluoxetine)
Fampridine (4 aminopyridines):
- Dose: 10 mg PO daily
3) Pain:
- Acute or chronic pain is a frequent complaint in MS patients affecting the quality of life
- Chronic pain description include burning, squeezing, lancinating or gritty
- Neuropathic pain does not respond to NSAIDs
Treatment:
Gabapentin:
- Dose: Begin at 100 to 300 mg PO TID
- Effective dose range: 900-1800 mg/daily in 3-4 divided doses
- Maximum dose: 2400-3600 mg/day
Carbamazepine:
- Dose: 100-200 mg PO daily
- Increase up to a total daily dosage of 600-1600 mg (divided) as tolerated
- Monitor drug levels, CBC, LFTs
Tramadol:
- Dose: 50-400 mg PO daily as tolerated
Pregabalin:
- Dose: May begin with 25-75 mg PO daily and increase to 150 mg PO BID
- Effective dose range: 900-1800 mg/daily in 3-4 divided doses
- Maximum dose: 600 mg daily in divided doses
Cannabinoids(delta-9-tetrahydrocannabinol & cannabidiol)
- Dose: Buccal 1 spray every 4 hr, 4-5 sprays/day for MS
- May start initially with 1 spray/day; increase every 1-2 days; Max. ~12 sprays/day
4) Paroxysmal symptoms:
- Lhermitte sign or barber chair phenomenon (an electrical sensation that radiates down the vertebra on flexion or extension of neck)
- Intermittent vertigo
Treatment:
- Carbamazepine
- Gabapentin
5) Bladder dysfunction:
Bladder spasticity:
- Oxybutynin: 5 mg PO TID or QID
- Tolterodine: 2 mg PO BID
- Imipramine: Usual dose 75 mg PO daily
- Solifenacin: 5 mg PO daily
- Darifenacin: Extended-release 7.5 mg PO daily; may increase to 15 PO daily
- Trospium: 20 mg PO BID
- Intravesicular botox: 200 Units
Denervated bladder treated by:
- Self-catheterization
Nocturia, night-time incontinence/urgency:
- Desmopressin (DDAVP): 0.1-0.4 mg PO once at bedtime
6) Bowel dysfunction:
Constipation: can be treated with the combination of fiber and stool softeners.
- High fiber diet and stool softeners
- Docusate Sodium: 100 mg PO TID
- Stimulants: Senna suppositories 2 tabs at bedtime; digital stimulation sometimes used
- Adopting a bowel regimen may help to regulate urges and incontinence
7) Sexual dysfunction
Erectile dysfunction:
Oral agents:
- Sildenafil* 50-100 mg
- Vardenafil* 5-20 mg
- Tadalafil* 5-20 mg
*Give medication 30 minutes prior to intercourse; caution advised in the elderly and with cardiac disease.
Injectable agents (intracavernous):
- Alprostadil:
- Begin with 2.5 mcg and titrate by 2.5 mcg increments
- Initial administered under the supervision
- Doses exceeding 40 mcg not recommended
Vaginismus:
- Antispasmodics
Vaginal dryness:
- Water-based lubrication
8) Depression
It can be managed through counseling and/or medication.
Tricyclic antidepressant
- Amitriptyline: 75-200 mg/day PO at night or in divided doses
- Imipramine: 75-150 mg/day PO at night or in divided doses
- Nortriptyline: 25-200 mg/day PO at night or in divided doses
Selective serotonin reuptake inhibitors (SSRIs)
- Fluoxetine: 20-80 mg PO once daily
- Paroxetine:
- 20 mg PO once daily
- May increase by 10 mg/day to a maximum of 50 mg/day
- Sertraline:
- 50 mg PO once daily
- Citalopram:
- 20 mg PO once daily; may increase by 20 mg/week to a maximum of 40 mg/day
Serotonin/norepinephrine reuptake inhibitors (SNRIs)
- Duloxetine:
- Start 30-60 mg PO once daily; target dose 60 mg/day
- May titrate dose by 30 mg/day if needed; Max. 120 mg/day
- Venlafaxine:
- Start 37.5-75 mg daily; may increase by 75 mg/day as tolerated
- Maximum 225 mg/day
Prognosis
- Variable and unpredictable
- If untreated, more than 50% of patients with multiple sclerosis will develop significant physical disability within 20-25 years from onset
- 70% of patients lead active, productive lives with prolonged remission
- 30% relapse in 1 year, 20% in 5-9 years, and 10% in 10-30 years
- Untreated MS Patients are thought to have an average life expectancy 5-7 years shorter than that of the general population
D) Non-pharmacological treatments
- Minimize exposure to exacerbating factors such as extreme temperature (hot tubs/saunas)
- A cooling vest or cold beverages may help lower body temperature
- Monitor for local sores and ulcers and take preventive measures before they become a source of infection
- Aerobic exercise may help prevent deconditioning
- Stretching exercises to help relieve stiffness
- Assistance with energy conserving techniques e.g. timed rest periods
- Bowel and bladder regimen to assist voiding; increase fiber and fluid intake
- Recommend self-catheterization where required
- Counseling: Psychologist, psychiatrist referral as required
[/cq_vc_tab_item][cq_vc_tab_item tabtitle=”Medication Dose”]MEDICATIONS:
ACUTE EXACERBATION-Medications
{kind=link}
- Methylprednisolone
- Prednisone
Use: Acute exacerbations
Mechanism:
- Decreases inflammation and the normal immune response through multiple mechanisms, also suppresses adrenal function in higher doses
Doses:
Methylprednisolone
- 1-2 g/day IV usually for 3-5 days (but can be used up to 10 days). Maybe followed by a tapering dose of oral prednisone (e.g. 100 mg x 1 dose then decrease by 10 mg daily until finished)
Prednisone
- 500-1000 mg PO daily for 3-5 days followed by tapering doses
DISEASE MODIFYING-Medications
{kind=link}
Types:
- Interferon Beta-1a (IFNb-1a)
- Interferon Beta-1b (IFNb-1b)
Use: Immunomodulating therapy
Mechanism:
- Exact mechanism in the treatment of MS is unknown
- Immunomodulatory effects include
- Enhancement of suppressor T cell activity
- Reduction of pro-inflammatory cytokines
- Down-regulation of antigen presentation
- Reduced trafficking of lymphocytes into the central nervous system
Dose:
Interferon Beta-1a (intramuscular)
- 30 µg once weekly
Note:
- Should be stored in a refrigerator at 2-8°C. Allow to reach room temperature (about 30 minutes) before giving the injection
- Prefilled syringe can be stored at room temperature (between 15-30°C) for up to one week
Interferon Beta-1a (subcutaneous)
- Titrate to 22-44 µg 3 times per week, at least 48 hours apart
- 44 µg titration: 8.8 µg 3 times per week for 2 wks; then 22 µg 3 times per week for 2 wks; followed by 44 µg 3 times per week
- 22 µg titration: Start 4.4 µg 3 times/week for 2 wks; then 11 µg 3 times/week for 2 wks; followed by 22 µg 3 times/week
Note: Interferon Beta-1a new HSA-free formulation liquid in a pre-filled syringe or pre-filled cartridge should be stored at 2-8°C. Allow warming to room temperature prior to use; do not use external heat sources such as hot water. It can also be stored for a limited time period at room temperature (up to 25°C), but not more than 1 month.
- Stored at 2-8°C. Allow to warm to room temperature prior to use, Do not use external heat sources such as hot water
- May be stored for a limited period at room temperature (up to 25°C), but not more than 1 month
General Care:
- Protect injection from light and do not freeze
- Rotate injection site with each injection, to minimize the likelihood of injection site reactions
- NSAIDs, acetaminophen may be used for flu-like symptoms
Interferon Beta-1b
Multiple sclerosis (relapsing)
- Titration: Increase by 0.0625 mg SC every 2 weeks as follows:
- Week 1-2 = 0.0625 mg every other day
- Week 3-4 = 0.125 mg every other day
- Week 5-6 = 0.1875 mg every other day
- Then 0.250 mg (target dose) every other day
Multiple sclerosis (secondary-progressive)
- Titration: 0.125 mg SC every other day for 2 weeks as follows; then 0.250 mg every other day
Note: Store between 2-25°C. After reconstitution, if not used immediately, refrigerate solution between 2 and 8°C and use within 3 hours of reconstitution.
{kind=link}
- Glatiramer acetate
Use: Immunomodulating therapy
Mechanism:
- Complete mechanism in the treatment of MS is unknown
- Supported hypothesis
- Induces and activate T-lymphocyte suppressor cells specific for a myelin antigen
- Interferes with the antigen-presenting function of certain immune cells opposing pathogenic T-cell function
Dose:
Glatiramer acetate:
- 20 mg SC once daily
- 40 mg SC 3 times per week
Sphingosine 1-phosphate receptor modulator
{kind=link}
- Fingolimod
Use: Immunomodulating therapy
Mechanism:
Complete mechanism in the treatment of MS is unknown
- Binds to sphingosine 1-phosphate (S1P) receptors 1, 3, 4, and 5
- It’s binding to S1P receptors on lymphocytes induces S1P receptor down-regulation on lymphocytes, and blocks the capacity of lymphocytes to egress from lymph nodes, reducing the number of lymphocytes in peripheral blood
- The amount of lymphocytes available to the central nervous system are decreased which reduces central inflammation
Dose:
Fingolimod:
- 0.5 mg PO once daily
Pyrimidine synthesis inhibitor
{kind=link}
- Teriflunomide
Use: Relapsing forms of multiple sclerosis (MS)
Mechanism:
Exact mechanism of action in MS is unknown
- An immunomodulatory agent that inhibits pyrimidine synthesis by inhibiting dihydroorotate dehydrogenase enzyme
- It also has anti-inflammatory effects
Dose:
Teriflunomide:
-
- 7 mg or 14 mg PO once daily (7 mg dose not available in Canada)
{kind=link}
{kind=link}
- Dimethyl Fumarate
Use: Treatment of adults with relapsing-remitting MS
Mechanism:
- Complete mechanism in the treatment of MS is unknown
- It is believed to result from its anti-inflammatory and cytoprotective properties via activation of the Nrf2 pathway
Dose:
Dimethyl Fumarate:
- Initiate 120 mg PO twice daily for 7 days; then increase to 240 mg PO twice daily
{kind=link}
- Alemtuzumab
Use: Adult RRMS
Mechanism:
- Binds to nucleic acids and inhibits DNA and RNA synthesis
- Replication is decreased by binding to DNA topoisomerase II
- Inhibit the incorporation of uridine into RNA and thymidine into DNA
- Active throughout entire cell cycle (cell-cycle nonspecific)
Dose:
Alemtuzumab:
- 300 mg IV once in 4 weeks
Selective adhesion molecule inhibitor
{kind=link}
- Natalizumab
Use: Immunomodulation therapy
Mechanism(s):
Complete mechanism in the treatment of MS is unknown.
- Binds integrins on leukocyte cell walls, preventing migration into inflamed parenchymal tissue (monoclonal antibody)
- Potentially blocks of T-lymphocyte migration into the CNS
Dose:
Natalizumab:
- 300 mg IV infusion over 1 hour every 4 weeks
Immune Modifiers/Monoclonal Antibody
{kind=link}
- Ocrelizumab
Use: Relapsing forms of multiple sclerosis (MS), to include
- Clinically isolated syndrome
- Relapsing-remitting disease
- Active secondary progressive
- Early Primary progressive MS
Mechanism:
- Selectively depletes CD20-expressing B cells
- B cells have been implicated in the pathogenesis of MS
- CD20 is a surface antigen found in pre-B cells and mature and memory B cells
Dose:
Ocrelizumab:
- Initial dose on day 1: 300 mg (in 250 ml) IV. Follow-up dose on day 15: 300 mg (in 250 ml) IV
- Maintenance: 600 mg (in 500 ml) IV every 6 months
NB: Premedicate 100 mg IV methylprednisolone (or alternative) and antihistamine (e.g. diphenhydramine), +/- Acetaminophen ~30 minutes prior to each infusion.
NB: All vaccines should be updated at least 4 weeks before starting treatment; hepatitis B screening required. Hepatitis B virus screening. Monitor for allergic reactions, rash, laryngeal edema, dyspnea, infections; increased risk of respiratory infections.
Immune Modifiers/ Sphingosine-1-phosphate receptor modulator
{kind=link}
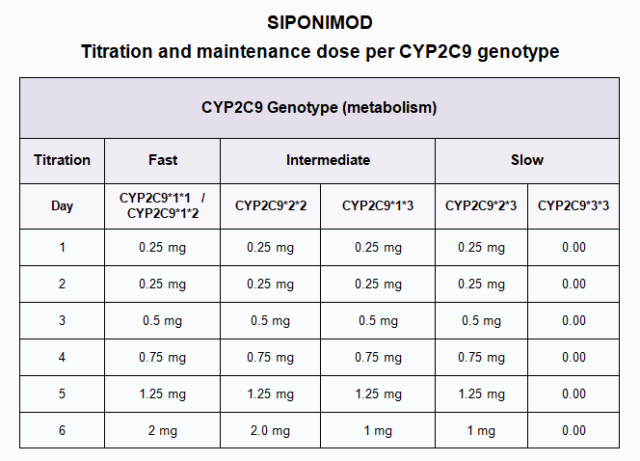
- Siponimod
Use: Secondary Progressive MS (SPMS) with active disease evidenced by relapses or imaging features characteristic of multiple sclerosis inflammatory activity.
Mechanism:
- Retention of lymphocytes (B cells and CD4+ and CD8+ T cells) within lymph nodes and thymus leading to ~ 20% to 30% reduction in circulating lymphocytes and hence reduced lymphocyte transition into the CNS
Dose:
Siponimod:
- Genotype dependent: Treatment is highly dependent on the CYP2C9 genotype defining those with fast, intermediate, or slow metabolizers. Consequently, CYP2C9 genotype needs to be established prior to initiation of treatment
- Assess past and present medical history, including diabetes, ophthalmological disease, concomitant use of immunosuppressive therapy, history of varicella-zoster and cardiac history including the use of antihypertensive agents
- There is a risk of cardiac anomalies including bradyarrhythmias, conduction block, and QTc prolongation that increases as enzyme metabolism decreases, hence the maintenance dose is reduced in intermediate and slow metabolizers and contraindicated in those with the slowest metabolizer genotype (CYP2C9*3*3). Obtain ECG prior to treatment to assess for pre-existing conduction abnormalities
Immune modifiers/Antineoplastic
{kind=link}
- Mitoxantrone
Use: Immunosuppressant therapy
Mechanism:
The mechanism by which it exerts its therapeutic effects in MS is not fully known.
- The drug may involve immunomodulation through the depletion and repopulation of lymphocytes
Dose:
Mitoxantrone:
- 5-12 mg/m2 IV every 3 months for 2 years, with maximum lifetime cumulative dose of 140 mg/m2
Antineoplastic/Immunosuppressant
{kind=link}
- Cyclophosphamide
Use: Immunosuppressant therapy
Mechanism:
- An alkylating agent that prevents cell division by cross-linking DNA strands and inhibiting DNA synthesis
- Interferes with DNA replication and RNA transcription
- It is a cell cycle phase, nonspecific agent and potent immunosuppressive agent
Dose:
Cyclophosphamide
Various treatment protocols exist for cyclophosphamide and methylprednisolone one of them stated below:
- 800 mg/m2 IV infusion given once every 4 weeks plus 1 g of methylprednisone. Dose adjustments based on preinfusion and 10 day post-infusion WBC
SYMPTOMATIC TREATMENT-Medications
{kind=link}
- Baclofen
- Tizanidine
- Cannabinoids
Use: Spasticity
Mechanism:
Complete mechanism of action unknown.
Baclofen
- It inhibits both monosynaptic and polysynaptic spinal reflexes, possibly by hyperpolarization of afferent terminals (resultant relief of muscle spasticity)
Tizanidine
- It is chemically-related to clonidine and other α2-adrenergic agonists, which acts as a centrally acting muscle relaxant with anti-hypertensive properties
- Presumably, it reduces spasticity by increasing presynaptic inhibition of motor neurons
Dose:
Baclofen
- 5-10 mg PO TID, may increase 5 mg/dose every 3 days; Max. 80 mg/day
Tizanidine
- 2-4 mg PO TID; may increase by 2-4 mg PO as needed to a maximum of 3 doses in 24 hrs, with at least 6-8 hrs interval between doses; Max. 36 mg/day
Dose in renal impairment:
- CrCl <25: Decrease dose (e.g. 2-4 mg PO)
Cannabinoids
- Buccal 1 spray every 4 hr, 4-5 sprays/day for MS, may start initially with 1 spray/day; increase every 1-2 d, Max ~12 sprays/day
{kind=link}
- Gabapentin
- Carbamazepine
{kind=link}
Use: Neuropathic pain, Lhermitte’s, Seizures
Mechanism:
Exact mechanism of action unknown.
- It is structurally related to GABA (gamma-aminobutyric acid)
- It does not affect the synthesis or uptake of GABA
- High-affinity gabapentin binding sites have been located throughout the brain
Dose:
Gabapentin
- Begin at 100 to 300 mg TID; increase as tolerated every 3-7 days. Effective dose range: 900-1800 mg daily in 3 divided doses. Max dose: 2400-3600 mg/day
Dose in renal impairment:
- CrCl 30-60: 200-700 mg twice daily
- CrCl 16-29: 200-700 mg once daily
- CrCl 15: 100-300 mg once daily
- CrCl <15: Decrease dose proportionately to creatinine clearance
- Hemodialysis: Single dose of 125-350 mg as a supplement every 4 hrs of dialysis
{kind=link}
Use: Neuropathic pain, Lhermitte’s, Seizures
Mechanism:
- Decreases synaptic transmission
- Within CNS by affecting sodium channels in neurons
- It had anticonvulsant, anticholinergic, antineuralgic, antidiuretic, muscle relaxant, antimanic, antidepressive, and antiarrhythmic properties
Dose:
Carbamazepine
- 100-200 mg/day PO; may increase up to a maximum of 600-1600 mg
- Monitor: CBC and risk of bone marrow suppression within the first 2 months of initiating therapy
{kind=link}
- Pregabalin
- Cannabinoids
Pregabalin
Primary use: Neuropathic pain may assist with Lhermitte’s; used for partial-onset seizures in some countries
Mechanism:
Exact mechanism of action is unknown.
- Binds to alpha2-delta subunit of voltage-gated calcium channels within the CNS, inhibiting excitatory neurotransmitter release
- Produces antinociceptive and antiseizure effects
Dose:
Pregabalin
- 75-150 mg PO BID; Max. dose 600 mg daily in 2-3 divided doses
{kind=link}
Cannabinoids
- Buccal 1 spray every 4 hr, 4-5 sprays/day for MS, may start initially with 1 spray/day; increase every 1-2 d, Max. ~12 sprays/day
{kind=link}
- Diazepam
Use: Spasticity, anxiety, sedation
Mechanism:
- Binds to benzodiazepine receptors and enhances GABA effects
- Depresses the CNS, produces skeletal muscle relaxation, has anticonvulsant properties due to enhanced presynaptic inhibition
Dose:
Diazepam
- 5-10 mg PO TID PRN; can be given as monotherapy or in combination
{kind=link}
- Amantadine
Use: Fatigue
Mechanism: Unclear
Dose:
Amantadine
- 100 mg PO BID; Max. 300 mg PO daily in divided doses
Central nervous system stimulant
{kind=link}
- Modafinil
Use: Fatigue in MS
Mechanism:
Exact mechanism of action is unknown.
- It may exert its stimulant effects by decreasing GABA-mediated neurotransmission
Dose:
Modafinil:
- 100 mg PO BID
Selective serotonin reuptake inhibitors (SSRIs)
{kind=link}
- Fluoxetine
Use: MS induced fatigue, depression
Mechanism:
- Inhibits the presynaptic reuptake of neurotransmitters and increases synaptic serotonin concentration and potentiates its effect
- Little effect on the reuptake of norepinephrine or dopamine
- Does not significantly bind to alpha-adrenergic, histamine, or cholinergic receptors
Dose:
Fluoxetine
- Start 20 mg/PO daily every morning; may increase dose gradually after several weeks if inadequate response; Max. 80 mg/day
{kind=link}
- Fampridine – Approved by Health Canada
- Dalfampridine – Approved by FDA
Use: Help to improve walking in patients with MS
Mechanism:
Exact mechanism of action is unknown.
- Inhibits potassium channels
- Delay repolarization and prolongs the duration of action potentials, improves conduction of action potentials in demyelinated axons
Dose:
Fampridine/Dalfampridine
- 10 mg PO every 12 hr
{kind=link}
- Tramadol
Use: Pain management
Mechanism:
The precise mechanism is unclear but may be related to:
- The binding of its active metabolites to mu-opioid receptors in the CNS which inhibits the reuptake of serotonin and norepinephrine
- The binding causes inhibition of ascending pain pathway which in turns alter the perception of and response to pain
Dose:
Tramadol
- 50-400 mg PO daily as tolerated
{kind=link}
- Oxybutynin
- Tolterodine
- Solifenacin
- Darifenacin
- Trospium
Use: Urinary incontinence
Mechanism:
- Antagonizes the action of acetylcholine at postganglionic receptors
- Relaxes bladder smooth muscle, inhibits involuntary detrusor muscle contractions
Dose:
Oxybutynin
- 5 mg PO BID or TID; Max. of 5 mg PO 4 times a day
Tolterodine
- 2 mg PO BID
Solifenacin
- 5 mg PO daily, if tolerated may increase to 10 mg once daily
- Note: Maximum 5 mg/day if on potent CYP3A4 inhibitor
Darifenacin
- 7.5 mg PO daily; may increase if required at least after 2 weeks to 15 mg PO daily
Trospium
- Immediate-release: 20 mg PO BID
- Extended-release: 60 mg PO daily
Neuromuscular blocking agent, (Botulinum toxin)
{kind=link}
- Botox
Use: Muscle spasticity, Urinary incontinence
Mechanism:
- Blocks neuromuscular conduction by binding to receptor sites on motor nerve terminals, inhibits the release of acetylcholine and produces a state of denervation that could last for weeks-months
Dose:
Botox (intramuscular)
- Exact dosage and number of injection sites are based on patient size, extent and location of muscles involved, severity of spasticity, presence of local muscle weakness, and response to prior treatment
Botox (intravesical)
- Recommended dose is 200 Units
- Treatment benefits usually last a minimum of three months.
{kind=link}
- Desmopressin
Use: Nocturia
Mechanism:
- Increases cyclic adenosine monophosphate (cAMP) in renal tubular cells with an increase in water permeability in distal tubules and collecting ducts leading to decreased urine volume and increased urine osmolality
- Increases plasma levels of von Willebrand factor, factor VIII, and t-PA
Dose:
Desmopressin
- 0.1-0.4 mg PO daily at bedtime
Antidepressants
- Tricyclic antidepressant (TCAs)
- Selective serotonin reuptake inhibitors (SSRIs)
- Serotonin/norepinephrine reuptake inhibitor (SNRIs)
Tricyclic antidepressants (TCAs)
{kind=link}
- Amitriptyline
- Imipramine
- Nortriptyline
Use: Depression
Mechanism:
- Inhibits the presynaptic reuptake of neurotransmitters, increases synaptic serotonin and/or norepinephrine
- Also has significant anticholinergic properties
Dose:
Amitriptyline
- Start 25-50 mg/day; may increase dose gradually; usual effective dose 75 to 200 mg PO daily or in divided doses; Max. 300 mg/day
Imipramine
- Start 75 mg/day and increase dose gradually to 150 mg PO daily or in divided doses; Max. 200 mg/day
Nortriptyline
- 25-50 mg/day PO; may increase gradually to 200 mg/day, if needed
Selective serotonin reuptake inhibitors (SSRIs)
{kind=link}
- Fluoxetine
- Paroxetine
- Sertraline
- Citalopram
Use: Depression
Mechanism:
- Inhibits the presynaptic reuptake of neurotransmitters, increases synaptic serotonin concentration
- Little effect on the reuptake of norepinephrine or dopamine
- Does not significantly bind to alpha-adrenergic, histamine, or cholinergic receptors
Dose:
Fluoxetine
- Start 20 mg PO daily in the morning; may increase dose gradually after several weeks if inadequate response; Max. 80 mg/day
Paroxetine
- Immediate-release: Start 20 mg PO daily in the morning; may increase dose gradually by 10 mg/day after at least 1 week of interval; Max. 50 mg/day
- Controlled-release (CR): Start 25 mg PO daily in the morning; may increase dose gradually by 12.5 mg/day after at least 1 week of interval; Max. 62.5 mg/day
Sertraline
- Start 50 mg PO in the morning or at bedtime once daily; may increase dose gradually after at least 1 week of interval; usual dose 50-100 mg/day; Max. 200 mg/day
Citalopram
- Start 20 mg PO in the morning or at bedtime once daily; may increase dose gradually after at least 1 week of interval; usual dose 20-40 mg/day; Max. 60 mg/day
Serotonin/Norepinephrine reuptake inhibitors (SNRIs)
{kind=link}
- Duloxetine
- Venlafaxine
Use: Depression, pain
Mechanism:
Exact mechanism of action is unknown.
- A potent serotonin and norepinephrine reuptake inhibitor
- Weakly inhibits dopamine reuptake
Dose:
Duloxetine
- 30-60 mg PO once daily; target dose 60 mg/day; may titrate dose by 30 mg/day if needed; Max. 120 mg/day
Venlafaxine
- 37.5-75 mg PO daily; may increase in ≤75 mg/day increments at intervals of ≥4 days as tolerated (maximum daily dose: 225-375 mg)
{kind=link}
- Docusate sodium
Use: Stool softener
Mechanism:
- Facilitates mixture of stool fat and water
- May also promote electrolyte and water secretion into the colon
Dose:
Docusate sodium
- 100 mg PO TID
Phosphodiesterase type 5 inhibitors (PDE5 inhibitors)
{kind=link}
- Sildenafil
- Tadalafil
- Vardenafil
Use: Erectile dysfunction
Mechanism:
- Does not directly cause penile erections
- Inhibits the enzyme phosphodiesterase type 5 (PDE5), which inactivates cGMP
- Enhances the effects of nitric oxide released during sexual stimulation
- Nitric oxide activates guanylatecyclase enzyme and increases cGMP level which leads to smooth muscle relaxation of corpus cavernosumhence promotes increased blood flow and subsequent erection
Dose:
Sildenafil
- 50-100 mg PO, prior to intercourse (~1 hour before)
Tadalafil
- 5-20 mg PO, prior to intercourse (at least 30 minutes)
Vardenafil
- 5-20 mg PO, prior to intercourse (~1 hour before)
{kind=link}
- Alprostadil
Use: Erectile dysfunction
Mechanism:
- Vasodilator – relaxes arterial smooth muscle and dilates cavernosal arteries
Dose:
Alprostadil
- 2.5-40 mg intracavernosal injection
[/cq_vc_tab_item][/cq_vc_tabs][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”clinical-trials-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Clinical Trials
[/vc_column_text][vc_column_text]
- Efficacy and Safety of Fingolimod in Patients With Relapsing-remitting Multiple Sclerosis (FREEDOMS)
- Oral Fingolimod or Intramuscular Interferon for Relapsing Multiple Sclerosis (TRANSFORM)
- Safety and Efficacy of Natalizumab in Combination With Interferon beta-1a in the Treatment of Multiple Sclerosis (SENTINEL)
- AFFIRM-A Randomized, Placebo-Controlled Trial of Natalizumab for Relapsing Multiple Sclerosis
- Effect of Mitoxantrone on MRI in progressive MS: results of the (MIMS trial)
- Intramuscular interferon beta-1a for disease progression in relapsing multiple sclerosis. The Multiple Sclerosis Collaborative Research Group (MSCRG).
- Interferon β-1a for early multiple sclerosis: CHAMPS trial subgroup analyses
- Effect of glatiramer acetate on conversion to (CDMS) in patients with clinically isolated syndrome
- Randomised study of interferon beta-1a in relapsing/remitting multiple sclerosis. PRISMS (Prevention of Relapses and Disability by Interferon beta-1a Subcutaneously in Multiple Sclerosis) Study Group.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”pipe-line-agents-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Pipeline Agents
[/vc_column_text][vc_column_text]
- Teriflunomide Successfully Reduces Relapses and is Well Tolerated in Multiple Sclerosis Patients
- Teriflunomide Oral in people With relapsing multiplEscleRosis (TOWER) Presented at 28th Congress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS). 2012, Abstract 153
- Oral Laquinimod for Multiple Sclerosis Treatment Significantly Reduced Disease Activity and Disability Progression While Providing Good Safety and Tolerability
- A Multinational, Multicenter, Randomized, Parallel-group Study Performed in Subjects With RRMS to Assess the Efficacy, Safety and Tolerability of Laquinimod Over Placebo in a Double-blind Design and a Reference Arm of Interferon β-1a (Avonex®) in a Rater-blinded Design
- Determination of the Efficacy and safety of oral Fumarate IN rElapsing-remitting MS
- Alemtuzumab versus interferon beta 1a as first-line treatment for patients with relapsing-remitting multiple sclerosis: a randomised controlled phase 3 trial
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”physician-resources-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Physician Resources
[/vc_column_text][vc_column_text]1. Tips for Patient Care
- Distinguish between new relapses and “pseudo exacerbations”; e.g. minor infections increase the risk of pseudo exacerbations
- Remissions can occur spontaneously, which make objective treatment evaluations difficult
- Additional MRIs may be indicated if there are new or unusual symptoms, or other unexpected clinical worsening, particularly for patients on natalizumab (Caveat: progressive multifocal leukoencephalopathy – PML)
- MS patients should receive regular care from a neurologist
- Advise the patient to establish a daily routine for medication use
- Consider starting lower doses in elderly and debilitated patients, to avoid undesired outcomes
- Consider comorbidities when prescribing medications
- Simplify medication regimen to improve compliance
Physical activity:
- Patients should maintain regular activity but avoid overwork and fatigue
- Advise rest during periods of acute relapse
- Hot climate/conditions may transiently worsen symptoms (Uhthoff’s phenomenon)
Social and Stress factors:
- Ensure patient and family members are well informed about the disease and its treatment
- Include family or social support in lifestyle modification
- Educate on the importance of self-catheterization for inadequate bladder emptying
- Suggest high fluid intake and a high-fiber diet to prevent or treat constipation
Expected outcome: Highly variable and unpredictable
- ~60-70% of patients lead active, productive lives with prolonged remissions
- Life expectancy of patients with MS is mildly reduced; average life expectancy ~5-7 years shorter than that of the general population
2. Scales and Tables
- 2010 McDonald criteria for the diagnosis of multiple sclerosis
- Symptoms often requiring attention in Multiple Sclerosis (MS)
- Comparison of Oral Disease-Modifying Therapies in MS
- Overview of Disease-Modifying Therapy in MS
- Kurtzke disability status scale
{kind=link}
{kind=link}
{kind=link}
{kind=link}
[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”references-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
References
[/vc_column_text][vc_column_text]Core Resources:
- Brust J, ed. Current Diagnosis and Treatment (Neurology). 2nd edition. New York: McGraw-Hill; 2011
- Compendium of Pharmaceuticals and Specialties (CPS). Canadian Pharmacist Association. Toronto: Webcom Inc. 2012
- Day RA, Paul P, Williams B, et al (eds). Brunner & Suddarth’s Textbook of Canadian Medical-Surgical Nursing. 2nd ed. Philadelphia: Lippincott Williams and Wilkins; 2010
- Foster C, Mistry NF, Peddi PF, Sharma S, eds. The Washington Manual of Medical Therapeutics. 33rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2010
- Freedman MS, Selchen D, Arnold DL, et al. Treatment Optimization in MS: Canadian MS Working Group Updated Recommendations. Can J Neurol Sci. 2013; 40(3):307-23
- Gray J, ed. Therapeutic Choices. Canadian Pharmacists Association. 6th ed. Toronto: Webcom Inc. 2011
- Katzung BG, Masters SB, Trevor AJ, eds. Basic and Clinical Pharmacology. 11th ed. New York: McGraw-Hill; 2009
- Longo D, Fauci A, Kasper D, et al (eds). Harrison’s Principles of Internal Medicine. 18thed. New York: McGraw-Hill; 2011
- McPhee SJ, Papadakis MA, eds. Current Medical Diagnosis & Treatment. 49th ed. New York: McGraw-Hill; 2010
- National Organization for Rare Diseases. Neuromyelitis Optica Spectrum Disorder, 2018. https://rarediseases.org/rare-diseases/neuromyelitis-optica/
- Rowland LP and Pedley TA, eds. Merritt’s Neurology. 12th ed. Philadelphia: Lippincott Williams and Wilkins; 2010
- Pagana KD, Pagana TJ eds. Mosby’s Diagnostic and Laboratory Test Reference. 9th ed. St. Louis: Elsevier-Mosby; 2009
- Siponimod Product Monograph, 2020, Novartis Pharmaceuticals Canada Inc.
- Skidmore-Roth L. ed. Mosby’s drug guide for nurses. 9th ed. St. Louis: Elsevier-Mosby; 2011
- Skidmore-Roth L, ed. Mosby’s nursing drug reference. 24th ed. St. Louis: Elsevier-Mosby; 2011
Online Pharmacological Resources:
- e-Therapeutics
- Lexicomp
- RxList
- Epocrates
Journals/Clinical Trials:
- Beck RW, Chandler DL, Cole SR, et al. Interferon β-1a for early multiple sclerosis: CHAMPS trial subgroup analyses. Annals of Neurology 2002;51:481-490
- Chapple CR, Kaplan SA, Mitcheson D et al. Randomized double-blind, active-controlled phase 3 study to assess 12-month safety and efficacy of mirabegron, a β(3)-adrenoceptor agonist, in overactive bladder. Eur Urol. 2013 63:296-305
- Cohen JA, Barkhof F, Comi G, et al. Oral fingolimod or intramuscular interferon for relapsing multiple sclerosis. N Engl J Med 2010;362:402-415
- Cohen JA, Coles AJ, Arnold DL, et al. Alemtuzumab versus interferon beta 1a as first-line treatment. Lancet. 2012;380(9856):1819-28. doi: 10.1016/S0140-6736(12)61769-3
- Comi G, Martinelli V, Rodegher M, et al. Affect of Glatiramer acetate on conversion to clinically definite multiple sclerosis (CDMS) in patients with clinically isolated syndrome (PreCISe study): a randomised, double-blind, placebo-controlled trial. Lancet. 2009;374:1503-11
- Ebers GC; PRISMS (Prevention of Relapses and Disability by Interferon beta-1a Subcutaneously in Multiple Sclerosis) Study Group. Randomized double-blind placebo-controlled study of interferon beta-1a in relapsing/remitting multiple sclerosis. Lancet.1998;352:1498-1504
- Gold R, Kappos L, Arnold DL, et al. Placebo-Controlled Phase 3 Study of Oral BG-12 for Relapsing Multiple Sclerosis. N Engl J Med 2012; 367:1098-1107
- Jacobs LD, Cookfair DL, Rudick RA, et al. The Multiple Sclerosis Collaborative Research Group (MSCRG). Intramuscular interferon beta-1a for disease progression in relapsing multiple sclerosis. Ann Neurol. 1996;393:285-94
- Kappos l, Bar-Or A, Cree BAC, et al. Siponimod versus placebo in secondary progressive multiple sclerosis (EXPAND): a double-blind, randomised, phase 3 study Lancet 2018; 391: 1263-1273
- Kappos L, O’Connor P, Radue EW. Long-term effects of fingolimod in multiple sclerosis: the randomized FREEDOMS extension trial. Neurology. 2015 Apr 14; 84:1582-91
- Kappos L, Radue EM, O’Connor P, et al. A Randomized, Placebo-Controlled Trial of Natalizumab for Relapsing Multiple Sclerosis. N Engl J Med 2006; 354:899-910
- Kappos L, Radue EM, O’Connor P, et al for the FREEDOMS Study Group. A placebo-controlled trial of oral fingolimod in relapsing multiple sclerosis. N Engl J Med 2010;362:387-401
- KHAN O, Rieckmann P, Boyko A, Selmaj K, et al. Three times weekly glatiramer acetate in relapsing-remitting multiple sclerosis. Ann Neurol. 2013;73:705–713
- Krapf H, Morrissey SP, Zenker O, et al. Effect of Mitoxantrone on MRI in progressive MS: results of the MIMS trial. Neurology. 2005;65:690-695
- Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology 1983;33:1444-52
- Lublin FD, Reingold SC, Cohen JA, et al. Defining the clinical course of multiple sclerosis: the 2013 revisions. Neurology. 2014;83(3):278-286. doi:10.1212/WNL.0000000000000560
- McDonald WI, Compston A, Edan G, et al. Recommended diagnostic criteria for multiple sclerosis: guidelines from the International Panel on the diagnosis of Multiple Sclerosis. Ann Neurol 2001;50:121-7
- Montalban X, Hauser SL, Kappos L, et al. Ocrelizumab versus Placebo in Primary Progressive Multiple Sclerosis. N Engl J Med. 2017;376(3):209-220. doi:10.1056/NEJMoa1606468
- Miller DH, Weinshenker BG, Filippi M, et al. Differential diagnosis of suspected multiple sclerosis: a consensus approach. Mult Scler. 2008;14(9):1157-74
- Rooney WD, Goodkin DE, Schuff N, et al. 1H MRSI of normal appearing white matter in multiple sclerosis. Mult Scler. 1997;3(4):231-7
- Rosati G. The prevalence of multiple sclerosis in the world: an update. Neurological Sciences 2001;22:117-139
- Rudick RA, Stuart WH, Calabresi PA, et al for the SENTINEL Investigators. Natalizumab plus interferon beta-1a for relapsing multiple sclerosis. N Engl J Med. 2006;354 (9):911-23
- Weinshenker BG, Wingerchuk DM. Neuromyelitis optica: clinical syndrome and the NMO-IgG autoantibody marker Curr Top Microbiol Immunol. 2008;318:343-56
[/vc_column_text][/vc_column_inner][/vc_row_inner][/vc_column][/vc_row]