[vc_row type=”full_width_content” full_screen_row_position=”middle” equal_height=”yes” content_placement=”middle” bg_color=”#ffffff” scene_position=”center” text_color=”light” text_align=”left” overlay_strength=”0.3″ shape_divider_position=”bottom” bg_image_animation=”none”][vc_column column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_link_target=”_self” column_shadow=”none” column_border_radius=”none” width=”1/1″ tablet_width_inherit=”default” tablet_text_alignment=”center” phone_text_alignment=”center” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”]
Asthma
[/vc_column_text][/vc_column_inner][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/3″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none” alignment=”right”][mpc_button preset=”mpc_preset_26″ url=”url:%23modal_id_reviewers|||” font_preset=”default” font_color=”#ffffff” font_size=”13″ font_line_height=”1.3″ font_transform=”uppercase” font_align=”right” title=”Reviewers” icon_size=”14″ background_color=”#555555″ border_css=”border-width:0px;border-color:#444444;border-style:solid;border-radius:3px;” padding_divider=”true” padding_css=”padding-top:8px;padding-right:8px;padding-bottom:8px;padding-left:8px;” margin_divider=”true” margin_css=”margin-top:10px;margin-right:2px;” hover_background_color=”#333333″ hover_border_css=”border-color:#444444;border-style:solid;”][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”none” text_align=”left” css=”.vc_custom_1565287910523{margin-top: -20px !important;}”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][mpc_button preset=”mpc_preset_26″ url=”url:%23modal_id_5ced944b48d3f|||” font_preset=”default” font_color=”#ffffff” font_size=”13″ font_line_height=”1.3″ font_transform=”uppercase” title=”Quick Review” icon_size=”14″ background_color=”#555555″ border_css=”border-width:0px;border-color:#444444;border-style:solid;border-radius:3px;” padding_divider=”true” padding_css=”padding-top:8px;padding-right:8px;padding-bottom:8px;padding-left:8px;” margin_divider=”true” margin_css=”margin-top:10px;margin-right:2px;” hover_background_color=”#333333″ hover_border_css=”border-color:#444444;border-style:solid;”][mpc_button preset=”mpc_preset_26″ url=”url:%23modal_id_video|||” font_preset=”default” font_color=”#ffffff” font_size=”13″ font_line_height=”1.3″ font_transform=”uppercase” title=”Lecture Slides” icon_size=”14″ background_color=”#555555″ border_css=”border-width:0px;border-color:#444444;border-style:solid;border-radius:3px;” padding_divider=”true” padding_css=”padding-top:8px;padding-right:8px;padding-bottom:8px;padding-left:8px;” margin_divider=”true” margin_css=”margin-top:10px;margin-right:2px;” hover_background_color=”#333333″ hover_border_css=”border-color:#444444;border-style:solid;”][mpc_button preset=”mpc_preset_26″ url=”url:%23modal_id_brochure|||” font_preset=”default” font_color=”#ffffff” font_size=”13″ font_line_height=”1.3″ font_transform=”uppercase” title=”Patient Brochure” icon_size=”14″ background_color=”#555555″ border_css=”border-width:0px;border-color:#444444;border-style:solid;border-radius:3px;” padding_divider=”true” padding_css=”padding-top:8px;padding-right:8px;padding-bottom:8px;padding-left:8px;” margin_divider=”true” margin_css=”margin-top:10px;margin-right:2px;” hover_background_color=”#333333″ hover_border_css=”border-color:#444444;border-style:solid;”][/vc_column_inner][/vc_row_inner][mpc_modal preset=”mpc_preset_5″ frequency=”onclick” onclick_id=”modal_id_5ced944b48d3f” max_width=”75″ max_height=”75″ position=”bottom-center” close_overlay=”true” mpc_icon__transition=”fade” mpc_icon__icon=”eti eti_close” mpc_icon__icon_color=”#555555″ mpc_icon__icon_size=”24″ mpc_icon__background_color=”#f3f3f3″ mpc_icon__border_css=”border-width:1px;border-color:#f3f3f3;border-style:solid;border-radius:99px;” mpc_icon__padding_css=”padding:10px;” mpc_icon__margin_divider=”true” mpc_icon__margin_css=”margin-top:-40px;margin-right:-40px;” mpc_icon__hover_icon_color=”#333333″ mpc_icon__hover_background_color=”#e5e5e5″ mpc_icon__hover_border_css=”border-width:5px;border-color:#e5e5e5;border-style:solid;border-radius:99px;” overlay_background_color=”rgba(48,48,48,0.48)” background_color=”#f7f7f7″ border_css=”border-width:15px;border-color:#e5e5e5;border-style:solid;” padding_css=”padding:40px;” animation_in_type=”transition.slideDownBigIn” animation_in_offset=”100″ animation_in_duration=”1200″ animation_in_delay=”1000″][vc_column_text]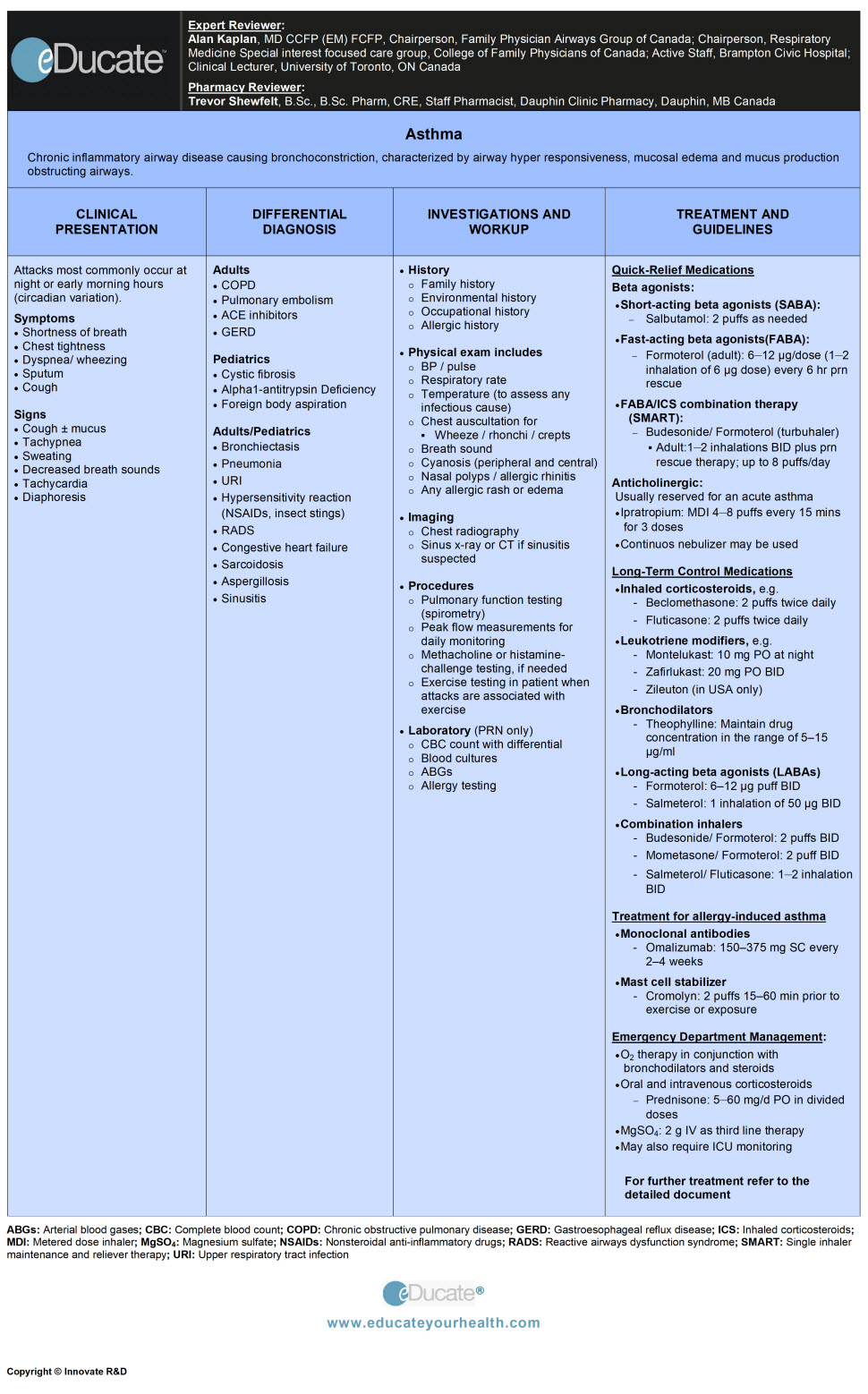 [/vc_column_text][/mpc_modal][mpc_modal preset=”mpc_preset_5″ frequency=”onclick” onclick_id=”modal_id_reviewers” max_width=”40″ max_height=”40″ mpc_icon__transition=”fade” mpc_icon__icon=”eti eti_close” mpc_icon__icon_color=”#555555″ mpc_icon__icon_size=”24″ mpc_icon__background_color=”#f3f3f3″ mpc_icon__border_css=”border-width:1px;border-color:#f3f3f3;border-style:solid;border-radius:99px;” mpc_icon__padding_css=”padding:10px;” mpc_icon__margin_divider=”true” mpc_icon__margin_css=”margin-top:-40px;margin-right:-40px;” mpc_icon__hover_icon_color=”#333333″ mpc_icon__hover_background_color=”#e5e5e5″ mpc_icon__hover_border_css=”border-width:5px;border-color:#e5e5e5;border-style:solid;border-radius:99px;” overlay_background_color=”rgba(48,48,48,0.48)” background_color=”#f7f7f7″ border_css=”border-width:15px;border-color:#e5e5e5;border-style:solid;” padding_css=”padding:40px;” animation_in_type=”transition.slideDownBigIn” animation_in_offset=”100″ animation_in_duration=”1200″ animation_in_delay=”1000″][vc_column_text]EXPERT REVIEWER:
[/vc_column_text][/mpc_modal][mpc_modal preset=”mpc_preset_5″ frequency=”onclick” onclick_id=”modal_id_reviewers” max_width=”40″ max_height=”40″ mpc_icon__transition=”fade” mpc_icon__icon=”eti eti_close” mpc_icon__icon_color=”#555555″ mpc_icon__icon_size=”24″ mpc_icon__background_color=”#f3f3f3″ mpc_icon__border_css=”border-width:1px;border-color:#f3f3f3;border-style:solid;border-radius:99px;” mpc_icon__padding_css=”padding:10px;” mpc_icon__margin_divider=”true” mpc_icon__margin_css=”margin-top:-40px;margin-right:-40px;” mpc_icon__hover_icon_color=”#333333″ mpc_icon__hover_background_color=”#e5e5e5″ mpc_icon__hover_border_css=”border-width:5px;border-color:#e5e5e5;border-style:solid;border-radius:99px;” overlay_background_color=”rgba(48,48,48,0.48)” background_color=”#f7f7f7″ border_css=”border-width:15px;border-color:#e5e5e5;border-style:solid;” padding_css=”padding:40px;” animation_in_type=”transition.slideDownBigIn” animation_in_offset=”100″ animation_in_duration=”1200″ animation_in_delay=”1000″][vc_column_text]EXPERT REVIEWER:
Alan Kaplan, MD CCFP (EM) FCFP, Chairperson, Family Physician Airways Group of Canada; Staff, Brampton Civic Hospital; Clinical Lecturer, University of Toronto, ON Canada
PHARMACY REVIEWER:
Trevor Shewfelt, B.Sc., B.Sc. Pharm, CRE, Staff Pharmacist, Dauphin Clinic Pharmacy, Dauphin, MB Canada[/vc_column_text][/mpc_modal][mpc_modal preset=”mpc_preset_5″ frequency=”onclick” onclick_id=”modal_id_brochure” max_width=”75″ max_height=”75″ position=”bottom-center” close_overlay=”true” mpc_icon__transition=”fade” mpc_icon__icon=”eti eti_close” mpc_icon__icon_color=”#555555″ mpc_icon__icon_size=”24″ mpc_icon__background_color=”#f3f3f3″ mpc_icon__border_css=”border-width:1px;border-color:#f3f3f3;border-style:solid;border-radius:99px;” mpc_icon__padding_css=”padding:10px;” mpc_icon__margin_divider=”true” mpc_icon__margin_css=”margin-top:-40px;margin-right:-40px;” mpc_icon__hover_icon_color=”#333333″ mpc_icon__hover_background_color=”#e5e5e5″ mpc_icon__hover_border_css=”border-width:5px;border-color:#e5e5e5;border-style:solid;border-radius:99px;” overlay_background_color=”rgba(48,48,48,0.48)” background_color=”#f7f7f7″ border_css=”border-width:15px;border-color:#e5e5e5;border-style:solid;” padding_css=”padding:40px;” animation_in_type=”transition.slideDownBigIn” animation_in_offset=”100″ animation_in_duration=”1200″ animation_in_delay=”1000″][vc_column_text]
[/vc_column_text][/mpc_modal][mpc_modal preset=”mpc_preset_5″ frequency=”onclick” onclick_id=”modal_id_video” max_width=”65″ max_height=”85″ mpc_icon__transition=”fade” mpc_icon__icon=”eti eti_close” mpc_icon__icon_color=”#555555″ mpc_icon__icon_size=”24″ mpc_icon__background_color=”#f3f3f3″ mpc_icon__border_css=”border-width:1px;border-color:#f3f3f3;border-style:solid;border-radius:99px;” mpc_icon__padding_css=”padding:10px;” mpc_icon__margin_divider=”true” mpc_icon__margin_css=”margin-top:-40px;margin-right:-40px;” mpc_icon__hover_icon_color=”#333333″ mpc_icon__hover_background_color=”#e5e5e5″ mpc_icon__hover_border_css=”border-width:5px;border-color:#e5e5e5;border-style:solid;border-radius:99px;” overlay_background_color=”rgba(48,48,48,0.48)” background_color=”#f7f7f7″ border_css=”border-width:15px;border-color:#e5e5e5;border-style:solid;” padding_css=”padding:40px;” animation_in_type=”transition.slideDownBigIn” animation_in_offset=”100″ animation_in_duration=”1200″ animation_in_delay=”1000″][vc_column_text]
[/vc_column_text][/mpc_modal][divider line_type=”Full Width Line” line_thickness=”1″ divider_color=”default” custom_height=”30″][/vc_column][/vc_row][vc_row type=”in_container” full_screen_row_position=”middle” scene_position=”center” text_color=”dark” text_align=”left” top_padding=”10″ class=”zindexbottom elementup” overlay_strength=”0.3″ shape_divider_position=”bottom” bg_image_animation=”none” shape_type=””][vc_column column_padding=”no-extra-padding” column_padding_position=”all” background_color=”#fcfcfc” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_link_target=”_self” column_shadow=”none” column_border_radius=”none” width=”1/1″ tablet_width_inherit=”default” tablet_text_alignment=”default” phone_text_alignment=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_row_inner column_margin=”default” text_align=”left” el_id=”definition-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Definition
[/vc_column_text][vc_column_text]Chronic inflammatory airway disease causing bronchoconstriction, characterized by airway hyperresponsiveness, mucosal edema and mucus production obstructing airways.[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”etiology-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Etiology
[/vc_column_text][vc_column_text]Interactions between susceptible genes and environmental factors play a role in the development of asthma.
- Susceptible genes and mediators involved include
- T-helper 1 and 2 (TH1 and TH2) cells, IgE, cytokines, GM-CSF
- Tumor necrosis factor-α (TNF-α)
- ADAM33 gene
- Environmental allergens include:
- Mold, pollen, dust mite and fungi
- Cockroaches and animal allergens
- Obesity (has been implicated)
- Work related asthma can be divided between
- Occupational asthma
- Work exacerbated asthma
- Allergic reactions to foods such as; peanuts, shellfish etc.
- Irritants: Such as household sprays, paint fumes, cigarette smoking, air quality (indoor and outdoor)
- Emotional factors or stress
- Perinatal factors: Pre-maturity, increased maternal age, maternal smoking and prenatal exposure to tobacco smoke
[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”epidemiology-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Epidemiology
[/vc_column_text][vc_column_text]
- Overall prevalence in Canadians
- Approx. 15.6% in under 12 years of age
- Approx. 8.3% in >12 years of age
- Asthma affects
- Approx. 2.2 million in Canadians
- Approx. 300 million persons worldwide
- Leading chronic illness in children
- Mortality rate of 20 children/year and 500 adults/year in Canada
- Leading cause of missed schools and third leading cause for sick day at work
- About 4000 asthma-related deaths annually in the US
[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”pathophysiology-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Pathophysiology
[/vc_column_text][vc_column_text]Gross pathology of asthmatic airways displays:
- Submucosal inflammation
- Lung hyperinflation
- Smooth muscle hypertrophy
- Mucosal edema
- Epithelial cell sloughing
- Mucus gland hypersecretion
Airflow obstruction is associated with:
- Acute bronchoconstriction
- Consequence of immunoglobulin E-dependent mediator and subsequent inflammation
- Directly mediated by some triggers such as cold air and exercise
- Airway edema
- Consequence of immunoglobulin E-dependent mediator
- Reaction to allergens
- Chronic mucous plug formation
- Exudate consists of serum proteins + Cell debris
- Airway remodeling is associated with structural changes
- Due to long-standing inflammation
- Long term scarring can affect reversibility of airway obstruction
{kind=link}
Inflammatory disorder of airways in which inflammation, airway remodeling, and hypersensitivity ultimately lead to bronchoconstriction and respiratory distress.[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”clinical-presentation-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Clinical Presentation
[/vc_column_text][vc_column_text]Asthma is a variable disease in which the symptoms wax and wane. Attacks occur most commonly at night or in early morning hours (circadian variation).
Mild to moderate attacks:
- Cough, dyspnea, and wheezing (with or without mucus production)
- Shortness of breath (prolonged expiratory phase)
- Increased respiratory rate (with use of accessory muscles)
- Chest tightness
- Decreased breath sounds
- Increased heart rate
- Decreased exercise tolerance
Life-threatening attacks: Include the above noted symptoms PLUS
- Peripheral cyanosis due to hypoxia as the attack progress
- Difficulty speaking
- Altered sensorium (with severe asthma attack)
 [/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”differential-diagnosis-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”differential-diagnosis-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Differential Diagnosis
[/vc_column_text][vc_column_text]Essentially a differential diagnosis for cough and wheeze in children and adults summarized as follows:
 [/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”investigation-and-workup-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”investigation-and-workup-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Investigation and Workup
[/vc_column_text][vc_column_text]Diagnosis:
Asthma can be diagnosed by history, physical exam and through objective measurements of pulmonary function in individuals ≥6 years and older.
Pulmonary function tests include:
- Spirometry (preferred)
- Measurements of lung function by spirometry, before and after administration of beta 2 agonists, should be used to confirm the clinical diagnosis of asthma (note, full pulmonary function testing is unnecessary)
- The ratio FEV1/FVC is a measure of airflow obstruction. Diagnosis of asthma is supported when reversible airflow obstruction is present
- Alternative studies include:
{kind=link}
{kind=link}
{kind=link}
In children <6 years of age (spirometry unavailable at this age) the diagnosis is suggested by:
- Typical pattern of coughing, wheezing, dyspnea
- Nighttime cough
- Exercise-induced symptoms
- Response to asthma drugs
- Absence of other medical conditions that might account for symptoms
History:
- History of presenting complaints: Breathlessness, wheezing, cough, sputum or chest tightness
- Exacerbation (frequency and severity)
- Triggers
- Smoking history
- Current treatment (e.g. steroid use)
- Psychosocial issues
- ER/Hospital visits
- Family history
- Environmental history
- Occupational history
- Allergic history
Physical Examination:
- Blood pressure, pulse, temperature, and respiratory rate
- Oximetry
- Chest auscultation for wheeze, rhonchi, and crepitations
- Breath sound reduction
- Nasal polyposis
- Cyanosis (peripheral and central)
- Any allergic rash or edema
- Accessory muscle use
- Hyperresponsiveness
- Pulsus paradoxus
Ref: Kaplan AG, Balter MS, Bell AD, et al. Diagnosis of asthma in adults. CMAJ November 10, 2009 vol. 181 no. 10 E210-E220.
Laboratory Studies:
Routine office/clinic visit may not require investigation if patient is stable.
Mild attack or at first presentation:
- Spirometry if >6 years
Consider ruling out concomitant issues or assessing triggers.
- CBC count with differential (eosinophilia >4% support asthma diagnosis)
- Chest radiography
- CT of sinuses (when chronic sinusitis a concern)
- Allergy testing
Moderate-severe exacerbations:
In addition to the workup for mild attacks, consider
- Blood cultures (if bacterial infection suspected)
- ABGs, if needed and concern for patient tiring in an acute attack
- Serum theophylline level, if taking theophylline
- Electrolytes with high dose B2 agonist use to rule out hypokalemia
[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”treatment-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Treatment
[/vc_column_text][cq_vc_tabs tabsstyle=”style2″ titlebg=”#16847d” titlehoverbg=”#333333″ rotatetabs=”0″][cq_vc_tab_item tabtitle=”Non-pharmacologic interventions”]
TREATMENT STRATEGIES:
CHRONIC ASTHMA:
A) Non-pharmacological measures
Education:
Goal:
- Enhance asthma knowledge to promote behavioral change, improve compliance and disease control
What is asthma?
- Information about what is asthma including airway inflammation and bronchospasm
Provocative factors/prevention:
- Identify and eliminate allergens
- Indoor: Animal fur/pets, house mites, cockroaches etc.
- Outdoor: Pollen, mold, etc.
- Air pollutants/irritants:
- Indoor: Smoking, carbon monoxide
- Outdoor: Aerosol, weather (humidity, thunderstorms)
- Work related asthma
- Work exacerbation asthma of preexisting disease
- Occupational asthma should be considered and investigated especially in adults with new-onset asthma
- Remove possible causative substance from exposure such as
- Certain foods and food additives
- Remove pets if necessary especially cats
- Old mattresses and pillow covers, if dust mite sensitive
- Emotional stress: May exacerbate asthma
- Drugs: Such as aspirin (and possible other NSAIDs) especially in those with nasal polyps
- Influenza vaccination: Does not protect against asthma exacerbations, but may prevent concomitant infections
- Pneumococcal vaccination: Literature is unclear on this, but there is a known higher risk of pneumococcal infections in those with asthma
Avoidance and adherence:
Patients should be made aware of:
- Underlying provocative factors and need for avoidance
- Correct use and side effects of preventive medications and bronchodilators
- Correct use of inhaler technique, and the need for regular follow-up
- Increasing medication for asthma control is not accounted as an avoidance strategy
Facilitation of asthma education and monitoring:
- Should be provided at each patient contact
- A written action plan for guided self-management (based on symptoms) should be provided to patients (e.g. www.AsthmaActionPlan.com; www.asthma-education.com)
- Communication and coordination between patients and health professionals is helpful to ensure the action plan is being followed
Home monitoring:
- Patients should be encouraged into self-monitoring of symptoms and/or use of PEF
- Symptom-based or PEF based monitoring appear to be similar in most cases
- PEF may be useful, especially for those who are poor perceivers of airflow obstruction
Physician office monitoring:
- Pattern and frequency of symptoms
- Nighttime attacks
- Exacerbations
- Monitoring the correct use of how and when to use medications
- Routine measurement of PEF
B) Pharmacological measures
- Relievers
- Controllers
Reliever medications:
- Used to relieve acute asthma symptoms
- Short-acting β2-agonists (SABA), are bronchodilators used on demand at minimum required dose and frequency
- Fast-acting β2 agonists (FABA), are bronchodilators that include fast acting medications with longer action e.g. formoterol
- For patients intolerant to Beta-agonists, inhaled ipratropium bromide may be used as a reliever (less effective than SABA)
Controller medications:
- Taken regularly to control asthma and prevent exacerbations
- Inhaled agents minimize systemic absorption and hence improves therapeutic benefit to the potential side-effects ratio
- Inhaled glucocorticosteroids (ICS) are the most effective agents in this category
Note: If reliever use >3 times per week or any other indicator of poor control presents then begin controller therapy (usually with low dose ICS) according to the recommended stepwise approach, by age as suggested.
- Control measures: Indicators of asthma control as assessed by the Canadian Thoracic Society (CTS)
- Recommended stepwise approach
- Treatment according to the age
{kind=link}
{kind=link}
{kind=link}
Follow-up and assessment are required in all patients:
Asthma is a chronic disease that requires regular follow up including:
- Assessing level of control; review of inhaler technique and effect on quality of life
- Frequency of follow up should be determined by the need to ensure good control of the disease
- Follow up 1-2 times per year may be adequate for those in good control
- Spirometry should be done to ensure diagnosis and then as a part of evaluation of asthma control, at least every 1-2 years
Considerations for special populations:
i) Elderly:
Asthma deaths in the elderly population account for more than 50% of asthma fatalities annually. Factors thought to contribute to such risk include:
- Delay in diagnosis and treatment
- Poor cardiorespiratory reserves
- Impaired perception of increasing airway obstruction
- Blunted hypoxic ventilatory drive
- Psychosocial problems
- Cognitive problems
Treatment options:
Approach is similar to that in younger subjects, however; an individualized approach may be required due to the existing comorbidities e.g.
- GERD is a common precipitant and mimic of asthma in elderly subjects
- Influenza and pneumococcal infections may complicate asthma exacerbations- vaccinations may help prevent infection-related to asthma exacerbations
- Use of spacers with inhalers or nebulizers may help improve drug delivery in the elderly
ii) Pregnancy:
- Treatment approach in pregnancy remains largely unaltered, however, LTRAs should be avoided unless necessary
- Goal is to strive for excellent asthma control
- Poorly controlled asthma results in increased perinatal mortality, prematurity and low birth rate
- Acute exacerbations should be treated promptly and aggressively to avoid fetal hypoxia
- Budesonide is the ‘safest’ ICS, with a pregnancy risk category of B (all others are C)
TREATMENT STRATEGY FOR ACUTE EXACERBATIONS
Treatment would be directed by the extent of the exacerbation which could be mild, moderate or severe.
In general:
- Oxygen: Should be titrated to achieve oxygen saturation of at least 92% whenever required
- Start high: FiO2 40-100% in adults and FiO2 100% in pediatric patients
- Inhaled β2-agonist and anticholinergic: Are used with doses titrated to the efficacy
- Systemic steroids should be utilized in the all but the mildest exacerbations, especially if:
- The initial rapid-acting inhaled β2-agonist therapy fails to achieve lasting improvement
- Development of exacerbation even though the patient was already on oral glucocorticoid
- Previous exacerbation required oral glucocorticoids
- Therapeutic approach to adult patients with mild, moderate and severe presentations
- Therapeutic approach to pediatric patients with mild, moderate and severe presentations
{kind=link}
{kind=link}
Follow-up management
Following acute exacerbation:
- Prescribe and encourage adequate regular SABA use for first 48 hrs then as required
- Oral steroid use for 7-14 days
- Reinforce patients’ knowledge about asthma and need for avoidance and compliance with their therapy
- Ensure patient is aware of acute signs and symptoms of an acute attack that may signify the need for urgent ED treatment
- Encourage regular follow-up visits with asthma clinic (where available), primary health care provider, as well as specialist (respirologist, pediatrician)
Outpatient monitoring (all asthmatics)
- The pattern of the symptoms (including nocturnal events and those with physical activity) should be documented
- Patient should diarize events including PEF, frequency, and dose of beta2-agonist
- Use of the inhalation device should be observed and corrected (if required)
- Perform and document spirometry (FEV1 and FEV1/FVC); testing should be done pre and post (~15 mins) inhaled beta2-agonist
[/cq_vc_tab_item][cq_vc_tab_item tabtitle=”Pharmacologic therapy”][/cq_vc_tab_item][cq_vc_tab_item tabtitle=”Medication Dose”] MEDICATIONS:
1) RELIEVER MEDICATIONS:
- Beta-agonists:
- Short-acting beta agonists (SABA)
- Fast-acting beta agonists (FABA)
- FABA/ICS combination therapy (SMART)
- Anticholinergic
Short/rapid-acting Beta-agonists (SABA):
{kind=link}
- Levalbuterol
- Salbutamol (Albuterol called in the USA)
- Terbutaline
Budesonide/Formoterol combination in maintenance and reliever strategy.
Mechanisms:
- Relaxes bronchial smooth muscle by action on beta2-receptors with little or no effect on a-adrenergic receptors
Dose:
Levalbuterol: not available in Canada
Adult:
Bronchospasm
- MDI: 2 puffs every 4-6 hrs
- Nebulizer: 0.63 mg TID at intervals of 6-8 hrs; may increase to 1.25 mg TID with close monitoring
Exacerbation of asthma
- MDI: 4-8 puffs every 20 mins for 4 hrs, then every 1-4hrs as needed
- Nebulizer: 1.25-2.5 mg every 20 min for 3 doses, then 1.25-5 mg every 1-4 hrs as needed
Pediatric:
Bronchospasm
- MDI: >4 years: Administer as in adults
- Nebulizer: <4 years: 0.31-1.25 mg every 4-6 hrs as needed; 5-11 years: 0.31 mg TID; Max. 0.63 mg TID
Exacerbation of asthma
- MDI: >4 years: 4-8 puffs every 20 mins for 3 doses, then every 1-4 hrs as needed prn
- Nebulizer: < 12 years: 0.075 mg/kg every 20 mins for 3 doses, then 0.075-0.15 mg/kg every 1-4 hrs as needed
Salbutamol (Albuterol in US):
Adult:
Bronchospasm
- Oral: 2-4 mg per dose divided in 2-3 doses/day: Max. 32 mg/day
- MDI: 2-3 puffs every 6 hrs. Max. 12 puffs/day; may use 2-4 puff every 20 min for 3 doses to treat an acute exacerbation
- Nebulizer: 2.5-5 mg every 4-6 hrs as needed, diluted in 2-5 ml sterile saline or water. Dilute 0.5 ml (2.5 mg) 0.5% inhalation solution in 1-2.5 ml of NS
Severe bronchospasm/Status asthmaticus:
- IV continuous infusion: Start 5 µg/min; may increase up to 10 µg/min & 20 µg/min at 5-30 ,minute intervals if needed
- Concentration should be reduced 50% before administration
Exacerbation of asthma
- MDI: 4-8 puffs every 20 min for up to 4hrs, then every 1-4 hrs as needed
- Nebulizer: 2.5-5 mg every 20 mins for 3 doses, then 2.5-10 mg every 1-4 hrs Or 10-15 mg/hr by continuous nebulization
Pediatric:
Bronchospasm
- Oral: 2-6 years: 0.1-0.2 mg/kg/dose PO TID daily; Max. 12 mg/day; age 6-12 years: 2 mg/dose PO TID or QID daily; Max. 24 mg/day
- MDI: <12 years: 2 puffs every 4-6 hrs; as needed with tube spacer; age >12 years: Same as above
- Nebulizer: 2-12 years: Nebulize 0.63-1.25 mg 3-4 times daily or as needed; age 12 years: Nebulize 2.5 mg 3-4 times daily as needed
Exacerbation of asthma
- MDI: <12 years: 4-8 puffs every 20 mins for 3 doses, then every 1-4hrs as needed; age ≥12 years: Administer as in adults
- Nebulizer: <12 years: 0.15 mg/kg every 20 mins for 3 doses, then 0.15-0.3 mg/kg every 1-4 hrs or 0.5 mg/kg/hour by continuous nebulization; age ≥12 years: Administer as in adults
FAST-acting beta agonists (FABA):
{kind=link}
- Formoterol
Mechanisms:
- These are the agents who have quick onset of action; and is effective for longer duration, so are often included in LABA
Dose:
- Adult: 6-12 µg/dose (1-2 inhalation of 6 µg dose) every 6 hr prn rescue (Canadian indication only)
{kind=link}
- Budesonide/Formoterol SMART strategy (only indicated in Canada with turbuhaler)
Mechanisms:
- Formoterol relaxes bronchial smooth muscle by action on beta2-receptors with little or no effect on a-adrenergic receptors. It has a quick onset of action
- Budesonide acts as an anti-inflammatory and immune modifier
Dose:
Adult
- 1- 2 inhalations BID plus prn rescue therapy; up to 8 puffs per day
Pediatric
- <12 years: Not established
- >12 years:1-2 inhalations BID plus prn rescue therapy (this is a second line therapy as data for children is much less than adults)
{kind=link}
- Ipratropium
Mechanisms:
- Inhibits cholinergic receptors in bronchial smooth muscle causing bronchodilator; local application to nasal mucosa inhibits secretions from glands lining the nasal mucosa
Dose:
Adult
- Nebulizer: 500 µg every 20 mins for 3 doses, then as needed for acute exacerbations
- MDI: 2 puffs QID; Max. 12 puffs/day
Pediatric
- Nebulizer: 250 µg TID
- MDI: 1-2 puffs TID; Max. 6 puffs/day
{kind=link}
- Methylprednisolone
- Hydrocortisone
- Prednisone
Mechanisms:
- Suppresses inflammation and the normal immune response, also suppresses adrenal function at high doses. It has minimal mineralocorticoid activity
Dose:
Methylprednisolone
- Adults: 125 mg/day IV in 2 divided doses
- Pediatric: 1-2 mg/kg/day IV in 2 divided doses
Hydrocortisone
- Adults: 250-500 mg IV in 4 divided doses/day
- Pediatric: 5-7 mg/kg/day IV divided every 12-24 hrs
Prednisone
- Adult: 40-60 mg PO daily divided in 2-4 doses; taper over 2 weeks as symptoms resolve
- Pediatric: <11 years: 1-2 mg/kg/day PO divided in 2-4 doses; taper over 2 weeks as symptoms resolve
Note: In asthma oral steroids are always preferred.
3) LONG-TERM CONTROL MEDICATIONS:
- Inhaled corticosteroids
- Leukotriene modifiers
- Bronchodilators
- Long-acting beta agonists (LABAs)
- Combination inhalers
{kind=link}
- Beclomethasone
- Budesonide
- Ciclesonide
- Fluticasone
- Mometasone
- Triamcinolone (not available in Canada)
Mechanisms:
- Acting as anti-inflammatory and immune modifier. May suppresses adrenal function at chronic high doses
Dose:
Beclomethasone
12 years of age and older:
- Mild Asthma: 50 to 100 µg twice daily; Max. 100 µg twice daily
- Moderate Asthma: 100 to 250 µg twice daily; Max. 500 µg twice daily
- More Severe Cases: 300 to 400 µg twice daily; Max. 800 µg twice daily
5-11 years of age:
- 50-100 µg twice daily; Max. 100 µg twice daily
Budesonide
- Adult: 400-2400 µg/day inhalation in 2-4 divided doses; maintenance is 200-400 µg twice daily
- Note: Patients taking only 400 µg/day may take it as a single daily dose
- Pediatric: Initially 200-400 µg/day inhalation in 2 divided doses; maintenance is individualized to lowest effective dose
Ciclesonide
12 years of age and older:
- Recommended initial dose 400 µg once daily; dose range 100-800 µg/day (1-2 puffs once daily either in the morning or evening); Max. 400 µg BID
6-11 years of age:
- Recommended initial dose 100-200 µg once daily; dose range 100-200 µg/day (1-2 puffs once daily either in the morning or evening); Max. 200 µg/day
Fluticasone
16 years of age and older:
- Mild Asthma: 100 to 250 µg BID
- Moderate Asthma: 250 to 500 µg BID
- Severe Asthma: 500 µg BID; may increase to 1000 µg BID to those patients currently requiring oral steroids
4-16 years of age:
- 50 or 100 µg BID daily; Max. 200 µg BID
12 months-4 years of age:
- 100 µg BID administered via a pediatric spacer device with a face mask
Mometasone:
12 years of age and older
- Usual recommended dose: 400 µg once daily in the morning or divided into BID; maintenance dose: 200-400 µg once daily in the morning
- Patients with severe asthma who may require oral corticosteroids: Starting dose: 400 µg twice daily; once reduction of oral steroid dose complete, titrate to the lowest effective dose
Triamcinolone
- Adult: 2 puffs 3-4 times a day or (400 µg) 4 sprays twice daily
- Pediatric: 6-12 years: 2 puffs 3-4 times a day or 2-4 puffs twice a day; >12 years: Administer as in adults
{kind=link}
- Montelukast
- Zafirlukast
- Zileuton (not available in Canada)
Mechanisms:
- Selective leukotriene receptor antagonist → inhibits the cysteinyl leukotriene receptor
- Have been correlated with the pathophysiology of asthma, including airway edema, smooth muscle contraction
Dose:
Montelukast
Prophylaxis and chronic treatment of asthma
- 15 years of age and older: 10 mg tablet once daily taken at evening time
- 6 to 14 Years of Age: 5 mg chewable tablet once daily at evening time
- 2 to 5 Years of Age: 4 mg chewable tablet or granules once daily at evening time
Zafirlukast
- ≥12 years of age: 20mg PO BID empty stomach; Max. 40 mg/day
Zileuton: (not available in Canada)
15 years of age and older:
- Immediate release: 600 mg four times/day
- Extended release: 1200 mg twice daily
{kind=link}
- Theophylline
Mechanisms:
- It increases tissue concentrations of cyclic adenosine monophosphate (cAMP), this in turns results in bronchodilation, CNS stimulation, positive inotropic and chronotropic effects, diuresis, and gastric acid secretion
Dose:
Theophylline
Adult:
- Initially 5-8 mg/kg/d IV to maintain concentration in the range of 5-15 µg/ml; then 5.6 mg/kg loading dose (based on aminophylline) IV over 20 min; followed by maintenance infusion of 0.1-1.1 mg/kg/hr
Pediatric:
- <6 weeks: Not established
- 6 weeks-to-6 months: 0.5 mg/kg/hr loading dose IV in first 12 hrs (based on aminophylline); followed by maintenance infusion of 12 mg/kg/d
- 6 months to 1 year: 0.6-0.7 mg/kg/hr loading dose IV in first 12 hrs; followed by maintenance infusion of 15 mg/kg/d
- >1 year: Administer as in adults
Long-acting beta agonists (LABA)
{kind=link}
- Formoterol
- Salmeterol
Mechanisms:
- Long acting control of reversible airway obstruction. It Relaxes bronchial smooth muscle by action on beta2-receptors with little or no effect on a-adrenergic receptors
Dose:
Formoterol
- Adult: 12 µg/day (1 inhalation) every 12 hr; Max. 48 µg/day
- Pediatric: <6 years: Not established; 6-16 years: Administer as in adults; Max. 24 µg/day
Salmeterol
- Adult: 1 inhalation (50 µg) BID ~12 hrs apart
- Pediatric: 4-12 years: 1 puff (50 µg) every 12 hrs; >12 years: Administer as in adults
{kind=link}
- Budesonide/Formoterol
- Mometasone/Formoterol
- Salmeterol/Fluticasone
Mechanisms:
- Formoterol, salmeterol relaxes bronchial smooth muscle by selective action on beta 2receptors with little effect on heart rate
- Formoterol has both a long-acting and rapid acting effect
- Fluticasone, budesonide and mometasone are corticosteroid which controls the rate of protein synthesis, depresses the migration of polymorphonuclear leukocytes/fibroblasts, and reverses capillary permeability and lysosomes stabilization at the cellular level to prevent or control inflammation
Dose:
Budesonide/Formoterol (100 µg/6 mcg per dose, 200 µg/6 µg per dose)
Only available as a turbuhaler in Canada and as MDI in USA.
Maintenance and reliever therapy
- 12 years and older: 1-2 inhalations twice daily or 2 inhalations once daily; may use additional 1 dose after every few minutes as needed up to maximum of 6 inhalations on any single occasion; Max. 8 inhalations total daily dose
Maintenance therapy
- Adults: 1-2 inhalations twice daily; Maximum recommended daily maintenance dose is 4 inhalations
- Pediatric: <12 years: Not established; >12 years: 1-2 inhalations once or twice daily
Note: In case of worsening asthma, may increase the dose temporarily up to 4 inhalations BID
Mometasone/Formoterol:
Maintenance treatment of asthma where combination therapy is indicated.
Mometasone 50 µg/formoterol 5 µg:
- 2 puffs twice daily; in patients previously on inhaled low dose corticosteroids; Max daily dose 200/20 µg (4 puffs)
Mometasone100 µg/formoterol 5 µg:
- 2 puffs twice daily; in patients previously on inhaled medium dose corticosteroids; Max daily dose 400/20 µg (4 puffs)
Mometasone 200 µg/formoterol 5 µg:
- 2 puffs twice daily; in patients previously on inhaled high dose corticosteroids; Max daily dose 800/20 µg (4puffs)
Salmeterol/Fluticasone (also available in an MDI in Canada)
- ➢ Diskus type is available in 3 strengths:
- Fluticasone/Salmeterol: 100 µg/50 µg, 250 µg/50 µg, 500 µg/50 µg
- ➢ Metered-dose inhaler (MDI) type is available in 2 strengths:
- Fluticasone/Salmeterol: 125 µg/25 µg, 250 µg/25 µg
Adult and Adolescents (≥12 years of age):
- Diskus (all strengths): One inhalation twice daily
- MDI (all strengths): Two inhalations twice daily
Note: If Diskus is used 2 puffs BID salmeterol overdose will ensue.
Pediatric (4-11 years of age):
- Fluticasone/Salmeterol (100 µg/50 µg): One inhalation twice daily
4) Treatment for allergy-induced asthma:
- Monoclonal antibodies
- Mast cell stabilizers
{kind=link}
- Omalizumab
Mechanisms:
- Inhibits IgE binding to receptors on mast cells and basophils. Prevents the release of mediators of the allergic response
Dose:
Omalizumab
- Adult: 150-375 mg SC every 3-4 weeks; inject slowly over 5-10 seconds due to viscosity. Not to exceed 150 mg/injection site
- Pediatric: <12 years: Not established; >12 years: Administer as in adults
{kind=link}
- Cromolyn
- Nedocromil
Mechanisms:
- Inhibits activation and release of mediators (e.g., histamine) from cells involved in hypersensitivity reactions (including mast cells). It inhibits the development of early and late bronchoconstriction responses to inhaled antigen
Dose:
Cromolyn
- Adult: 2 puffs 15-60 min prior to exercise or exposure
- Pediatric: <12 years: Not established; ≥12 years: Administer as in adults
Nedocromil
- 2 inhalations 4 times/day; may reduce dosage to 2-3 times/day once desired clinical response to initial dose is observed
[/cq_vc_tab_item][/cq_vc_tabs][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”clinical-trials-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Clinical Trials
[/vc_column_text][vc_column_text]
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”pipe-line-agents-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Pipeline Agents
[/vc_column_text][vc_column_text]
{kind=link}
[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”physician-resources-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Physician Resources
[/vc_column_text][vc_column_text]1. Tips for Patient Care
Risk factor management:
- Promote smoking Cessation – Cigarette smoking leads to frequent hospitalizations and higher risk of death from asthma
- Food allergies and sulfites (in food and wine) may precipitate symptoms
- If occupational exposure is suspected, details of job and workplace environment should be accounted and evaluated
- Patient should be aware of asthma symptoms and therapy
- Compare symptom history; at and away from work
Education:
{kind=link}
Medications:
Day to day maintenance
- If patients require oral corticosteroid treatment for maintenance then monitor:
- Bone density and established preventive treatment as required
- Blood glucose levels
- Blood pressure
- They should be referred on for a specialist assessment
- Abrupt discontinuation of systemic glucocorticoids may cause adrenal crisis
- Simplify medication regimen to improve compliance
- Use sufficient doses to get asthma under control then taper down after 6-12 weeks once control established
- Aspirin sensitivity and nasal polyps affect 5-10% of patients with asthma (there may be some advantage to consideration of LTRAs in this population
- Consider concurrent comorbidities with the prescribed therapy
- Patient should understand how to deal with asthma worsening (Ref: Balter M, Ernst P, Watson W, Kaplan A, et al. Asthma worsenings. Approaches to prevention and management from the Asthma Worsenings Working group. Can Respir J 2008;15(Suppl B):1B-19B)
During a moderate to severe exacerbation of asthma:
- Avoid aggressive hydration in older children and adults, and monitor electrolytes
- Monitor serum levels in patients taking theophylline
- Antibiotics are prescribed only during acute exacerbations if signs and symptoms of bacterial infection are present
Social and stress factors:
- Include family or social support in lifestyle modification
- Avoid circumstances leading to stress
- Patient should recognize the early signs and symptoms of anaphylaxis (if applicable) and loss of asthma control
Physical activity:
- Regular aerobic exercise should be encouraged
- Adaptive breathing techniques and breathing exercises such as pursed-lip breathing
2. Scales and Table
{kind=link}
[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”references-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
References
[/vc_column_text][vc_column_text]Core Resources:
- Balter MS, Bell AD, Kaplan AG et al. Management of asthma in adults. CMAJ. 2009 8; 12:915-22
- Chapman KR, McIvor A. Asthma that is unresponsive to usual care. CMAJ 2010 182:45-52
- Compendium of Pharmaceuticals and Specialties (CPS). Canadian Pharmacist Association. Toronto: Webcom Inc. 2012
- Day RA, Paul P, Williams B, et al (eds). Brunner & Suddarth’s Textbook of Canadian Medical-Surgical Nursing. 2nd ed. Philadelphia: Lippincott Williams and Wilkins; 2010
- FitzGerald JM, Boulet L-P, McIvor RA, et al. Asthma control in Canada remains suboptimal: The Reality of Asthma Control (TRAC) study Can Respir J. 2006 Jul-Aug; 13(5): 253-259
- Foster C, Mistry NF, Peddi PF, Sharma S, eds. The Washington Manual of Medical Therapeutics. 33 rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2010
- Gray J, ed. Therapeutic Choices. Canadian Pharmacists Association. 6th ed. Toronto: Webcom Inc. 2011
- Guidelines for the Diagnosis and Management of Asthma. National Asthma Education and Prevention Programme Expert Panel Report 3. NIH Publication Number 08-5846. 2007
- Hodder R, Lougheed MD, Rowe BH et al. Management of acute asthma in adults in the emergency department: nonventilatory management. A.CMAJ. 2009
- DOI:10.1503/cmaj.080072
- Horne R, Price D, Cleland J, et al. Can asthma control be improved by understanding the patient’s perspective. BMC Pulmonary Medicine 2007, 7:8
- DOI:10.1186/1471-2466-7-8
- Kaplan A. Action Plans in Asthma. The (Canadian) Family Physician, August 2002
- Kaplan AG, Balter MS, Bell AD, et al. Diagnosis of asthma in adults. CMAJ 2009;181(10):E210-E220
- Katzung BG, Masters SB, Trevor AJ, eds. Basic and Clinical Pharmacology. 11th ed. New York: McGraw-Hill; 2009
- Kovesi T, Schuh S, Spier S et al. Achieving control of asthma in preschoolers .CMAJ 2010; 4:E175
- Longo D, Fauci A, Kasper D, et al (eds). Harrison’s Principles of Internal Medicine. 18thed. New York: McGraw-Hill; 2011
- Lougheed MD, Lemiere C, Ducharme FM et al. Canadian Thoracic Society 2012 guideline updates: Diagnosis and management of asthma in preschoolers, children and adults. Can Respir J 2012; 19:127-164
- McPhee SJ, Papadakis MA, eds. Current Medical Diagnosis & Treatment. 49th ed. New York: McGraw-Hill; 2010
- Pagana KD, Pagana TJ eds. Mosby’s Diagnostic and Laboratory Test Reference. 9th ed. St. Louis: Elsevier-Mosby; 2009
- Skidmore-Roth L. ed. Mosby’s drug guide for nurses. 9th ed. St. Louis: Elsevier-Mosby; 2011
- Skidmore-Roth L, ed. Mosby’s nursing drug reference. 24th ed. St. Louis: Elsevier-Mosby; 2011
- Online resource/weblinks:
- The Children’s Asthma Education Centre (CAEC)
- The Family Physicians Airway Group of Canada (FPAGC)
- The National Heart, Lung, and Blood Institute (NHLBI)
Online Pharmacological Resources:
- e-Therapeutics
- Lexicomp
- RxList
- Epocrates
Journals/Clinical Trials:
- Abramson MJ, Puy RM, Weiner JM. Is allergen immunotherapy effective in asthma? A meta-analysis of randomized controlled trials. Am J Respir Crit Care Med. Apr 1995; 151:969-74
- Bacci E, Cianchetti S, Bartoli M, et al. Low sputum eosinophils predict the lack of response to beclomethasone in symptomatic asthmatic patients. Chest. 2006; 3:565-72
- Bailey WC, Richards JM Jr, Brooks CM, Soong SJ, Windsor RA, Manzella BA. A randomized trial to improve self-management practices of adults with asthma. Arch Intern Med. 1990; 8:1664-8
- Barnes PJ. Inhaled glucocorticoids for asthma. N Engl J Med.1995; 13:868-75
- Burrows B, Barbee RA, Cline MG, Knudson RJ, Lebowitz MD. Characteristics of asthma among elderly adults in a sample of the general population. Chest. Oct 1991;100(4):935-42
- Busse WW, Calhoun WF, Sedgwick JD. Mechanism of airway inflammation in asthma. Am Rev Respir Dis. 1993;147:S20-4
- Camargo CA Jr, Weiss ST, Zhang S, Willett WC, Speizer FE. Prospective study of body mass index, weight change, and risk of adult-onset asthma in women. Arch Intern Med. Nov 22 1999; 21:2582-8
- Castro M, Rubin AS, Laviolette M, et al. Effectiveness and safety of bronchial thermoplasty in the treatment of severe asthma: a multicenter, randomized, double-blind, sham-controlled clinical trial. Am J Respir Crit Care Med. 2010; 2:116-24
- Cates CJ, Lasserson TJ, Jaeschke R. Regular treatment with formoterol and inhaled steroids for chronic asthma: serious adverse events. Cochrane Database Syst Rev. 2009; CD006924
- Centers for Disease Control and Prevention. Asthma–United States, 1982-1992. MMWR Morb Mortal Wkly Rep. 1995;51-52:952-5
- Chan-Yeung M. 2003 Christie Memorial lecture. Occupational asthma–the past 50 years. Can Respir J. 2004;1:21-6
- Chan-Yeung M. Assessment of asthma in the workplace. ACCP consensus statement. American College of Chest Physicians. Chest. 1995; 4:1084-117
- Coffman JM, Cabana MD, Yelin EH. Do school-based asthma education programs improve self-management and health outcomes? Pediatrics. 2009; 2:729-42
- Crapo RO, Casaburi R, Coates AL, et al. Guidelines for Methacholine and exercise challenge testing-1999. This official statement of the American Thoracic Society was adopted by the ATS Board of Directors, 1999. Am J Respir Crit Care Med. 2000;1:309-29
- Dell S, To T, Breastfeeding and Asthma in Young Children: Title and subTitle Break Findings From a Population-Based Study. Arch Pediatr Adolesc Med. 2001; 155:1261-1265
- Djukanovic R, Wilson JW, Britten KM, et al. Effect of an inhaled corticosteroid on airway inflammation and symptoms in asthma. Am Rev Respir Dis. 1992; 3:669-74
- Dombrowski MP, Schatz M. ACOG practice bulletin: clinical management guidelines for obstetrician-gynecologists number 90, February 2008: asthma in pregnancy. Obstet Gynecol. 2008; 2 Pt 1: 457-64
- doi: 10.1097/AOG.0b013e3181665ff4
- Enright PL, Lebowitz MD, Cockroft DW. Physiologic measures: pulmonary function tests. Asthma outcome. Am J Respir Crit Care Med. 1994; 2 Pt 2 :S9-18; S19-20
- Green RH, Brightling CE, McKenna S, et al. Asthma exacerbations and sputum eosinophil counts: a randomised controlled trial. Lancet. 2002; 9347:1715-21
- Hamilos DL. Gastroesophageal reflux and sinusitis in asthma. Clin Chest Med. 1995; 4:683-97
- Harding SM, Guzzo MR, Richter JE. The prevalence of gastroesophageal reflux in asthma patients without reflux symptoms. Am J Respir Crit Care Med. 2000; 1:34-9
- Harding SM, Sontag SJ. Asthma and gastroesophageal reflux. Am J Gastroenterol. 2000; 8:S23-32
- Henderson WR Jr. Role of leukotrienes in asthma. Ann Allergy.1994; 3:272-8
- Horwitz RJ, Busse WW. Inflammation and asthma. Clin Chest Med. 1995; 4:583-602
- Ignacio-Garcia JM, Gonzalez-Santos P. Asthma self-management education program by home monitoring of peak expiratory flow. Am J Respir Crit Care Med.1995; 2 Pt 1:353-9
- Irwin RS, Curley FJ, French CL. Chronic cough. The spectrum and frequency of causes, key components of the diagnostic evaluation, and outcome of specific therapy. Am Rev Respir Dis. 1990; 141:640-7
- Juniper EF, Buist AS, Cox FM, Ferrie PJ, King DR. Validation of a standardized version of the Asthma Quality of Life Questionnaire. Chest.1999; 5:1265-70
- Kiljander TO, Salomaa ER, Hietanen EK, Terho EO. Gastroesophageal reflux in asthmatics: A double-blind, placebo-controlled crossover study with omeprazole. Chest.1999; 5:1257-64
- Kingston HG, Hirshman CA. Perioperative management of the patient with asthma. Anesth Analg. 1984; 9:844-55
- Kotses H, Bernstein IL, Bernstein DI, et al. A self-management program for adult asthma. Part I: Development and evaluation. J Allergy Clin Immunol. 1995; 2:529-40
- Lahdensuo A, Haahtela T, Herrala J, et al. Randomised comparison of guided self-management and traditional treatment of asthma over one year. BMJ.1996; 7033:748-52
- Laitinen LA, Laitinen A, Haahtela T. A comparative study of the effects of an inhaled corticosteroid, budesonide, and a beta 2-agonist, terbutaline, on airway inflammation in newly diagnosed asthma: a randomized, double-blind, parallel-group controlled trial. J Allergy Clin Immunol. 1992; 1:32-42
- McFadden ER Jr. Exercise-induced airway obstruction. Clin Chest Med. 1995; 4:671-82
- Martin AJ, Landau LI, Phelan PD. Lung function in young adults who had asthma in childhood. Am Rev Respir Dis.1980; 4:609-16
- Morris MJ, Deal LE, Bean DR, Grbach VX, Morgan JA. Vocal cord dysfunction in patients with exertional dyspnea. Chest. 1999; 6:1676-82
- Nair P, Pizzichini MM, Kjarsgaard M, et al. Mepolizumab for prednisone-dependent asthma with sputum eosinophilia. N Engl J Med. 2009; 10:985-93
- Nathan RA, Sorkness CA, Kosinski M, et al. Development of the asthma control test: a survey for assessing asthma control. J Allergy Clin Immunol. 2004; 1:59-65
- National Asthma Education and Prevention Program. Expert Panel Report 2: Guidelines for the diagnosis and management of asthma. NIH Publication No. 97-4051. NIH Publication. 1997
- National Asthma Education and Prevention Program. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. NIH Publication No. 07-4051. 2007
- National Asthma Education and Prevention Program Expert Panel Report 3, Guidelines for the Diagnosis and Management of Asthma. No. 08-5846 Washington DC: NIH, Oct 2007
- National Heart, Lung, and Blood Institute. Global Strategy for Asthma Management and Prevention. NIH Publication. 2008
- National Heart, Lung, and Blood Institute. Measures of asthma assessment and monitoring. Expert panel report 3: guidelines for the diagnosis and management of asthma. National Asthma Education and Prevention Program (NAEPP). 2007
- National Heart, Lung, and Blood Institute. NAEPP Working Group Report: Considerations for Diagnosing and Managing Asthma in the Elderly. NIH Publication No. 96-3662. National Institutes of Health; 1996
- National Heart, Lung, and Blood Institute. Executive Summary: Management of Asthma During Pregnancy. NIH Publication No. 92-3279a. National Institutes of Health; 1992
- Nayak A. A review of montelukast in the treatment of asthma and allergic rhinitis. Expert Opin Pharmacother. 2004; 3:679-86
- Nelson HS. Advair: combination treatment with fluticasone propionate/salmeterol in the treatment of asthma. J Allergy Clin Immunol. 2001; 2:398-416
- O’Byrne PM, Parameswaran K. Pharmacological management of mild or moderate persistent asthma. Lancet. 26 2006; 9537:794-803
- Randolph C. Exercise-induced asthma: update on pathophysiology, clinical diagnosis, and treatment. Curr Probl Pediatr. 1997; 2:53-77
- Reddel HK, Taylor DR, Bateman ED, et al. An official American Thoracic Society/european Respiratory Society statement: asthma control and exacerbations: standardizing endpoints for clinical asthma trials and clinical practice. Am J Respir Crit Care Med. 1 2009; 1:59-99
- Rowe BH, Keller JL, Oxman AD. Effectiveness of steroid therapy in acute exacerbations of asthma: a meta-analysis. Am J Emerg Med. 1992; 4:301-10
- Rowe BH, Edmonds ML, Spooner CH, Diner B, Camargo CA Jr. Corticosteroid therapy for acute asthma. Respir Med. 2004; 4:275-84
- Sears MR. Consequences of long-term inflammation. The natural history of asthma. Clin Chest Med. 2000; 2:315-29
- Sly RM. Changing asthma mortality. Ann Allergy.1994;3:259-68.
- Smith AD, Cowan JO, Brassett KP, Herbison GP, Taylor DR. Use of exhaled nitric oxide measurements to guide treatment in chronic asthma. N Engl J Med. 26 2005; 21:2163-73
- Strunk RC, Weiss ST, Yates KP, Tonascia J, Zeiger RS, Szefler SJ. Mild to moderate asthma affects lung growth in children and adolescents. J Allergy Clin Immunol. 2006;5:1040-7
- Suissa S, Ernst P, Boivin JF, et al. A cohort analysis of excess mortality in asthma and the use of inhaled beta-agonists. Am J Respir Crit Care Med. Mar 1994; 3 Pt 1:604-10
- Woolcock A, Lundback B, Ringdal N, Jacques LA. Comparison of addition of salmeterol to inhaled steroids with doubling of the dose of inhaled steroids. Am J Respir Crit Care Med.1996;15:1481-8
- Wenzel SE, Covar R. Update in Asthma 2005. Am J Resp Crit Care 2006; 173:698-706
- Williams SG, Schmidt DK, Redd SC, Storms W. Key clinical activities for quality asthma care. [Guideline] Recommendations of the National Asthma Education and Prevention Program. MMWR Recomm Rep. 2003;52:1-8
[/vc_column_text][/vc_column_inner][/vc_row_inner][/vc_column][/vc_row]