[vc_row type=”full_width_content” full_screen_row_position=”middle” equal_height=”yes” content_placement=”middle” bg_color=”#ffffff” scene_position=”center” text_color=”light” text_align=”left” overlay_strength=”0.3″ shape_divider_position=”bottom” bg_image_animation=”none”][vc_column column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_link_target=”_self” column_shadow=”none” column_border_radius=”none” width=”1/1″ tablet_width_inherit=”default” tablet_text_alignment=”center” phone_text_alignment=”center” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”]
Acute Coronary Syndrome (ACS)
[/vc_column_text][/vc_column_inner][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/3″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none” alignment=”right”][mpc_button preset=”mpc_preset_26″ url=”url:%23modal_id_reviewers|||” font_preset=”default” font_color=”#ffffff” font_size=”13″ font_line_height=”1.3″ font_transform=”uppercase” font_align=”right” title=”Reviewers” icon_size=”14″ background_color=”#555555″ border_css=”border-width:0px;border-color:#444444;border-style:solid;border-radius:3px;” padding_divider=”true” padding_css=”padding-top:8px;padding-right:8px;padding-bottom:8px;padding-left:8px;” margin_divider=”true” margin_css=”margin-top:10px;margin-right:2px;” hover_background_color=”#333333″ hover_border_css=”border-color:#444444;border-style:solid;”][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”none” text_align=”left” css=”.vc_custom_1565287910523{margin-top: -20px !important;}”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][mpc_button preset=”mpc_preset_26″ url=”url:%23modal_id_5ced944b48d3f|||” font_preset=”default” font_color=”#ffffff” font_size=”13″ font_line_height=”1.3″ font_transform=”uppercase” title=”Quick Review” icon_size=”14″ background_color=”#555555″ border_css=”border-width:0px;border-color:#444444;border-style:solid;border-radius:3px;” padding_divider=”true” padding_css=”padding-top:8px;padding-right:8px;padding-bottom:8px;padding-left:8px;” margin_divider=”true” margin_css=”margin-top:10px;margin-right:2px;” hover_background_color=”#333333″ hover_border_css=”border-color:#444444;border-style:solid;”][mpc_button preset=”mpc_preset_26″ url=”url:%23modal_id_video|||” font_preset=”default” font_color=”#ffffff” font_size=”13″ font_line_height=”1.3″ font_transform=”uppercase” title=”Lecture Slides” icon_size=”14″ background_color=”#555555″ border_css=”border-width:0px;border-color:#444444;border-style:solid;border-radius:3px;” padding_divider=”true” padding_css=”padding-top:8px;padding-right:8px;padding-bottom:8px;padding-left:8px;” margin_divider=”true” margin_css=”margin-top:10px;margin-right:2px;” hover_background_color=”#333333″ hover_border_css=”border-color:#444444;border-style:solid;”][mpc_button preset=”mpc_preset_26″ url=”url:%23modal_id_brochure|||” font_preset=”default” font_color=”#ffffff” font_size=”13″ font_line_height=”1.3″ font_transform=”uppercase” title=”Patient Brochure” icon_size=”14″ background_color=”#555555″ border_css=”border-width:0px;border-color:#444444;border-style:solid;border-radius:3px;” padding_divider=”true” padding_css=”padding-top:8px;padding-right:8px;padding-bottom:8px;padding-left:8px;” margin_divider=”true” margin_css=”margin-top:10px;margin-right:2px;” hover_background_color=”#333333″ hover_border_css=”border-color:#444444;border-style:solid;”][/vc_column_inner][/vc_row_inner][mpc_modal preset=”mpc_preset_5″ frequency=”onclick” onclick_id=”modal_id_5ced944b48d3f” max_width=”75″ max_height=”75″ position=”bottom-center” close_overlay=”true” mpc_icon__transition=”fade” mpc_icon__icon=”eti eti_close” mpc_icon__icon_color=”#555555″ mpc_icon__icon_size=”24″ mpc_icon__background_color=”#f3f3f3″ mpc_icon__border_css=”border-width:1px;border-color:#f3f3f3;border-style:solid;border-radius:99px;” mpc_icon__padding_css=”padding:10px;” mpc_icon__margin_divider=”true” mpc_icon__margin_css=”margin-top:-40px;margin-right:-40px;” mpc_icon__hover_icon_color=”#333333″ mpc_icon__hover_background_color=”#e5e5e5″ mpc_icon__hover_border_css=”border-width:5px;border-color:#e5e5e5;border-style:solid;border-radius:99px;” overlay_background_color=”rgba(48,48,48,0.48)” background_color=”#f7f7f7″ border_css=”border-width:15px;border-color:#e5e5e5;border-style:solid;” padding_css=”padding:40px;” animation_in_type=”transition.slideDownBigIn” animation_in_offset=”100″ animation_in_duration=”1200″ animation_in_delay=”1000″][vc_column_text]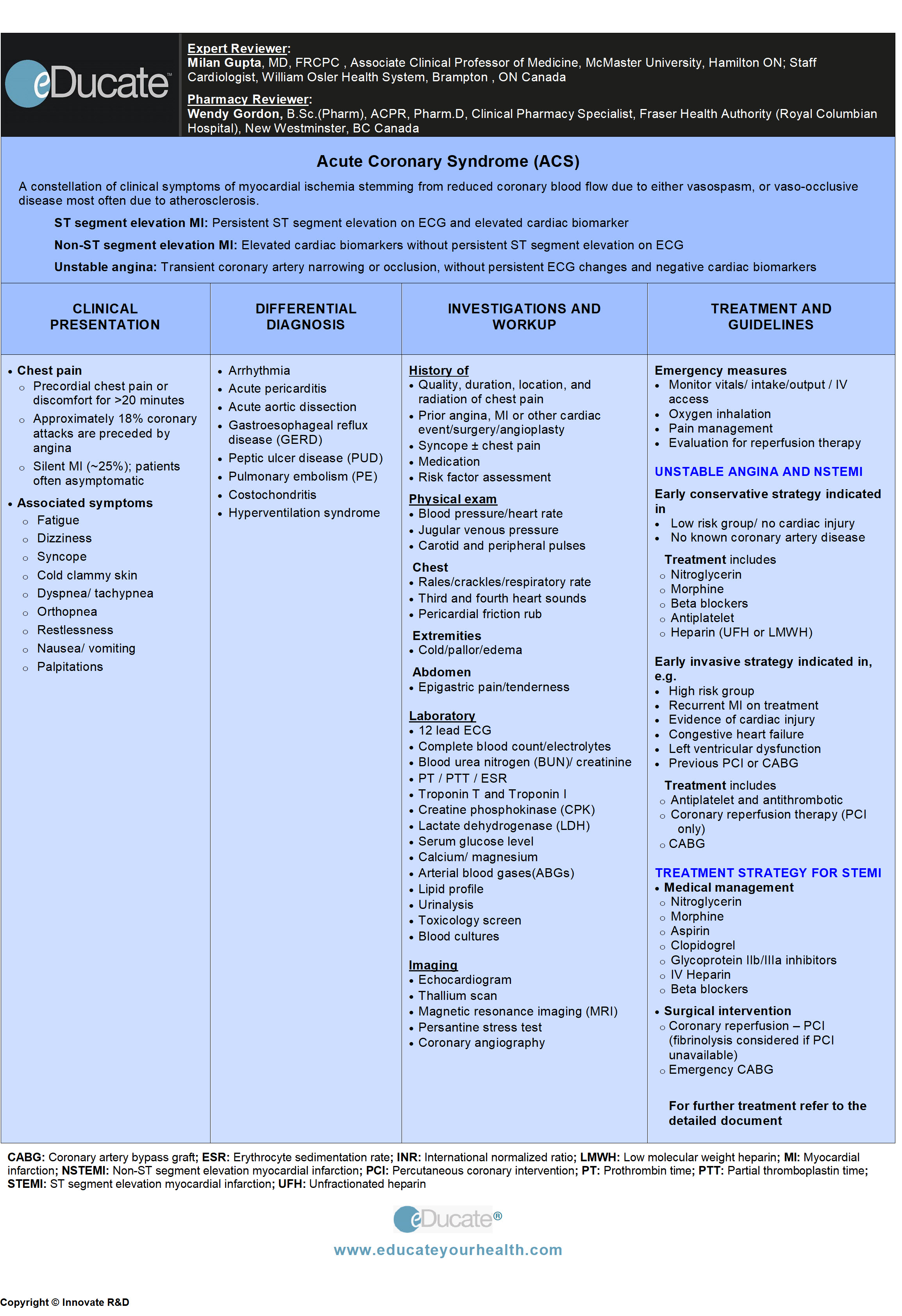 [/vc_column_text][/mpc_modal][mpc_modal preset=”mpc_preset_5″ frequency=”onclick” onclick_id=”modal_id_reviewers” max_width=”40″ max_height=”40″ mpc_icon__transition=”fade” mpc_icon__icon=”eti eti_close” mpc_icon__icon_color=”#555555″ mpc_icon__icon_size=”24″ mpc_icon__background_color=”#f3f3f3″ mpc_icon__border_css=”border-width:1px;border-color:#f3f3f3;border-style:solid;border-radius:99px;” mpc_icon__padding_css=”padding:10px;” mpc_icon__margin_divider=”true” mpc_icon__margin_css=”margin-top:-40px;margin-right:-40px;” mpc_icon__hover_icon_color=”#333333″ mpc_icon__hover_background_color=”#e5e5e5″ mpc_icon__hover_border_css=”border-width:5px;border-color:#e5e5e5;border-style:solid;border-radius:99px;” overlay_background_color=”rgba(48,48,48,0.48)” background_color=”#f7f7f7″ border_css=”border-width:15px;border-color:#e5e5e5;border-style:solid;” padding_css=”padding:40px;” animation_in_type=”transition.slideDownBigIn” animation_in_offset=”100″ animation_in_duration=”1200″ animation_in_delay=”1000″][vc_column_text]EXPERT REVIEWER:
[/vc_column_text][/mpc_modal][mpc_modal preset=”mpc_preset_5″ frequency=”onclick” onclick_id=”modal_id_reviewers” max_width=”40″ max_height=”40″ mpc_icon__transition=”fade” mpc_icon__icon=”eti eti_close” mpc_icon__icon_color=”#555555″ mpc_icon__icon_size=”24″ mpc_icon__background_color=”#f3f3f3″ mpc_icon__border_css=”border-width:1px;border-color:#f3f3f3;border-style:solid;border-radius:99px;” mpc_icon__padding_css=”padding:10px;” mpc_icon__margin_divider=”true” mpc_icon__margin_css=”margin-top:-40px;margin-right:-40px;” mpc_icon__hover_icon_color=”#333333″ mpc_icon__hover_background_color=”#e5e5e5″ mpc_icon__hover_border_css=”border-width:5px;border-color:#e5e5e5;border-style:solid;border-radius:99px;” overlay_background_color=”rgba(48,48,48,0.48)” background_color=”#f7f7f7″ border_css=”border-width:15px;border-color:#e5e5e5;border-style:solid;” padding_css=”padding:40px;” animation_in_type=”transition.slideDownBigIn” animation_in_offset=”100″ animation_in_duration=”1200″ animation_in_delay=”1000″][vc_column_text]EXPERT REVIEWER:
Milan Gupta, MD, FRCPC, Associate Clinical Professor of Medicine, McMaster University, Staff Cardiologist, William Osler Health System, Brampton, ON Canada
PHARMACY REVIEWER:
Wendy Gordon, B.Sc.(Pharm), ACPR, Pharm.D, Coordinator, Clinical Pharmacy Services, Fraser Health, Provincial Health Services Authority, BC Canada[/vc_column_text][/mpc_modal][mpc_modal preset=”mpc_preset_5″ frequency=”onclick” onclick_id=”modal_id_brochure” max_width=”75″ max_height=”75″ position=”bottom-center” close_overlay=”true” mpc_icon__transition=”fade” mpc_icon__icon=”eti eti_close” mpc_icon__icon_color=”#555555″ mpc_icon__icon_size=”24″ mpc_icon__background_color=”#f3f3f3″ mpc_icon__border_css=”border-width:1px;border-color:#f3f3f3;border-style:solid;border-radius:99px;” mpc_icon__padding_css=”padding:10px;” mpc_icon__margin_divider=”true” mpc_icon__margin_css=”margin-top:-40px;margin-right:-40px;” mpc_icon__hover_icon_color=”#333333″ mpc_icon__hover_background_color=”#e5e5e5″ mpc_icon__hover_border_css=”border-width:5px;border-color:#e5e5e5;border-style:solid;border-radius:99px;” overlay_background_color=”rgba(48,48,48,0.48)” background_color=”#f7f7f7″ border_css=”border-width:15px;border-color:#e5e5e5;border-style:solid;” padding_css=”padding:40px;” animation_in_type=”transition.slideDownBigIn” animation_in_offset=”100″ animation_in_duration=”1200″ animation_in_delay=”1000″][vc_column_text]
[/vc_column_text][/mpc_modal][mpc_modal preset=”mpc_preset_5″ frequency=”onclick” onclick_id=”modal_id_video” max_width=”65″ max_height=”85″ mpc_icon__transition=”fade” mpc_icon__icon=”eti eti_close” mpc_icon__icon_color=”#555555″ mpc_icon__icon_size=”24″ mpc_icon__background_color=”#f3f3f3″ mpc_icon__border_css=”border-width:1px;border-color:#f3f3f3;border-style:solid;border-radius:99px;” mpc_icon__padding_css=”padding:10px;” mpc_icon__margin_divider=”true” mpc_icon__margin_css=”margin-top:-40px;margin-right:-40px;” mpc_icon__hover_icon_color=”#333333″ mpc_icon__hover_background_color=”#e5e5e5″ mpc_icon__hover_border_css=”border-width:5px;border-color:#e5e5e5;border-style:solid;border-radius:99px;” overlay_background_color=”rgba(48,48,48,0.48)” background_color=”#f7f7f7″ border_css=”border-width:15px;border-color:#e5e5e5;border-style:solid;” padding_css=”padding:40px;” animation_in_type=”transition.slideDownBigIn” animation_in_offset=”100″ animation_in_duration=”1200″ animation_in_delay=”1000″][vc_column_text]
[/vc_column_text][/mpc_modal][divider line_type=”Full Width Line” line_thickness=”1″ divider_color=”default” custom_height=”30″][/vc_column][/vc_row][vc_row type=”in_container” full_screen_row_position=”middle” scene_position=”center” text_color=”dark” text_align=”left” top_padding=”10″ class=”zindexbottom elementup” overlay_strength=”0.3″ shape_divider_position=”bottom” bg_image_animation=”none” shape_type=””][vc_column column_padding=”no-extra-padding” column_padding_position=”all” background_color=”#fcfcfc” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_link_target=”_self” column_shadow=”none” column_border_radius=”none” width=”1/1″ tablet_width_inherit=”default” tablet_text_alignment=”default” phone_text_alignment=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_row_inner column_margin=”default” text_align=”left” el_id=”definition-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Definition
[/vc_column_text][vc_column_text]A constellation of clinical symptoms of myocardial ischemia stemming from reduced coronary blood flow due to either vasospasm or vaso-occlusive disease most often due to atherosclerosis.
Classified as:
- ST-segment elevation myocardial infarction: Acute occlusion of coronary blood supply with persistent ST-segment elevation on ECG and elevated cardiac biomarkers
- Non-ST segment elevation myocardial infarction: Transient partial coronary artery narrowing with raised cardiac biomarkers and without persistent ST-segment elevation
- Unstable angina (UA): Transient coronary artery narrowing or occlusion, without persistent ECG changes and negative cardiac biomarkers
[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”etiology-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Etiology
[/vc_column_text][vc_column_text]
- Atherosclerotic coronary artery disease
- Coronary emboli / spasm
- Dissection of the aorta or coronary arteries
- Vasoconstricting agents or illicit drugs e.g. cocaine
RISK FACTORS
Non-modifiable:
- Age
- Men ≥50 years
- Women ≥60 years
- Gender
- Male > Female
- History of vascular disease (coronary artery disease, stroke, peripheral vascular disease)
- Family history of premature (<55 years) vascular disease
- Ethnicity
Modifiable:
- Hypertension
- Hyperlipidemia
- Cigarette smoking
- Diabetes mellitus
- Obesity / abdominal obesity
- Metabolic syndrome
- Sedentary lifestyle
- Hypercoagulability
- Stress
FRAMINGHAM RISK ASSESSMENT
Used to determine the most appropriate treatment for managing cholesterol in patients without overt vascular disease or high-risk diabetes.
The risk factors included in the Framingham calculation are:
- Age
- Total cholesterol
- High-density lipoprotein (HDL) cholesterol
- Systolic blood pressure – not treated
- Systolic blood pressure – treated
- Smoking
- Diabetes
The modified total cardiovascular Framingham Risk Score is now recommended in Canada
- Low risk is defined as individuals with an FRS of less than 10%
- Intermediate is defined as individuals with an FRS of 10% to 19%
- High risk is defined as individuals with an FRS of 20% or greater
Indication for Screening:
Suggested screening with a full lipid profile, every 1 to 3 years for the following:
- Males ≥ 40 years
- Females ≥ 50 years or who are post-menopausal
In addition, adults with the following risk factors should be screened at any age:
- Diabetes mellitus
- Hypertension
- Cigarette smoking
- Obesity (body mass index greater than 27 kg/m2)
- Calculate BMI = weight in kilograms / (height in meter)2
- Central Obesity:
- Family history of premature coronary artery disease (CAD)
- Clinical signs of hyperlipidemia
- Erectile dysfunction
- Estimated glomerular filtration rate of less than 60 mL/min/1.73 m2
- Evidence of atherosclerosis
- Rheumatoid arthritis, systemic lupus erythematosus, psoriasis
- HIV infection on highly active antiretroviral therapy
{kind=link}
{kind=link}
Ref: Genest J. et al. Can J Cardiol 2009; 25(10):567-579.[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”epidemiology-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Epidemiology
[/vc_column_text][vc_column_text]Canada:
- Prevalence: 1.3 million Canadians are living with heart disease
- Incidence of MI: Approximately 70,000/year
- Deaths due to MI: Approximately 16,000/year
- Hospitalizations due to ischemic heart disease: Approximately 160,000/year
USA:
- Prevalence: Approximately 17 million diagnosed with coronary artery disease (CAD)
- Incidence of first MI: Approximately 785,000/year
- Incidence of all MI (first, recurrent or silent): Approximately 1.45 million/year
- Hospitalizations due to ischemic heart disease: Approximately 1.6 million/year
- Ratio of unstable angina:MI = ~60:40
- Ratio of NSTEMI:STEMI = ~70:30
[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”pathophysiology-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Pathophysiology
[/vc_column_text][vc_column_text]Atherosclerosis within coronary vessels underlies the main trigger for acute coronary syndrome (ACS).
Mechanism:
- Low-density lipoprotein (LDL) particles penetrate the endothelium → initiate atherosclerosis by recruiting macrophages → inflammation and increased plaque growth over time
- Plaque rupture → platelet aggregation → thrombus → partial or complete vessel occlusion → decrease oxygenation → myocardial hypoxia → ischemia/infarction
- If untreated, the ensuing area of necrosis continues to spread. Completely blocked coronary arteries may cause full thickness injury/infarction (STEMI), while partial occlusion causes non-full thickness myocardium injury (NSTEMI)
 [/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”clinical-presentation-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”clinical-presentation-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Clinical Presentation
[/vc_column_text][vc_column_text]Chest pain:
- Precordial chest pain or discomfort for >20 minutes
- Approx. 18% of coronary attacks are preceded by angina
- Silent MI (~25%); patients often asymptomatic
Associated symptoms:
- Lightheadedness / dizziness / fatigue
- Restlessness / palpitations
- Nausea / vomiting
- Dyspnea / tachypnea / orthopnea
- Cold clammy skin
- Syncope
[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”differential-diagnosis-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Differential Diagnosis
[/vc_column_text][vc_column_text]Arrhythmia:
- Palpitations, lightheadedness, dizziness, fainting and/or shortness of breath
Acute pericarditis:
- Sharp, piercing chest pain that is positional, relieves by sitting up
Acute aortic dissection:
- Sudden excruciating precordial or interscapular pain, syncope and widened mediastinum on x-ray chest
Gastroesophageal reflux disease (GERD):
- Chest pain of burning type, with the metallic taste in mouth, may be associated with food intake, regurgitation of food
Peptic ulcer disease (PUD):
- Epigastric pain with severity relating to mealtimes, dyspepsia, bloating, nausea/vomiting, loss of appetite and weight loss
Pulmonary embolism (PE):
- Sudden-onset of shortness of breath with pleuritic chest pain, tachypnea, and cough
Costochondritis:
- Pain and tenderness is usually worsened by activity, exercise and deep breathing
Hyperventilation syndrome:
- Chest pain, lasting for hours rather than minutes and relieved by exercise than being provoked, may present with or without tachypnea, dyspnea, wheezing, palpitations, muscle spasms, suffocation, dry mouth and lightheadedness
[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”investigation-and-workup-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Investigation and Workup
[/vc_column_text][vc_column_text]HISTORY
- Quality, duration, location, and radiation of chest pain, occurring at rest or on exertion
- Prior history of angina, myocardial infarction or other cardiac events/surgery/angioplasty
- History of syncope ±chest pain
- Medication history
- Risk factor assessment
- Diabetes mellitus
- Hypertension
- Cerebrovascular disease
- Bleeding / coagulative disorders
- Smoking
- Alcohol and drug use/ abuse (specially cocaine)
PHYSICAL EXAM
a) Vital signs
- Heart rate
- Blood pressure (BP)
- Respiratory rate
b) Assess chest for
- Tenderness / third and fourth heart sounds
- Rales / crackles
- Pericardial friction rub
c) Extremities: Cold / pallor / edema
d) Neck: Jaw tenderness / elevated JVP / pain radiating to the jaw and/or shoulder
e) Abdomen: Epigastric pain / guarding
LABORATORY
a) 12 lead ECG
{kind=link}
- T wave changes reflect myocardial ischemia
- ST-segment elevation reflects myocardial injury
- If infarction occurs, the ST segment may return to baseline within hours
- New Q waves appear within hours to days → signifies previous MI
- Q-waves may persist for the lifetime
b) Cardiac biomarkers
Troponins have largely replaced CPK and LDH
Troponin T (TnT) and Troponin I (TnI):
Most sensitive test for myocardial infarction.
- Rises: 3-6 hours
- Peaks: 18-24 hours
- Values increase over time:
- Normal: 0.00-0.24 µg/L
- Equivocal: >0.24-0.40
- Duration: TnI = 5-10 days; TnT = 0-14 days
- Troponin I (more specific than troponin T)
Other (less commonly used biomarkers):
- Creatine phosphokinase (CPK)
- Lactic dehydrogenase (LDH)
c) Complete blood count (CBC)/ESR
d) PT / PTT / INR
e) BUN/creatinine
f) Serum electrolytes
g) Serum and urine glucose level
h) Liver function tests (LFTs)
i) Arterial blood gases (ABGs)
{kind=link}
- Should be checked within 24 hrs of acute coronary syndrome (ACS) to avoid acute phase reactant effect
k) Urinalysis
l) Toxicology screen
m) Blood cultures: (if infection is suspected)
IMAGING
Imaging should not delay implementation of reperfusion therapy (unless a potential contraindication, such as suspected aortic dissection).
Chest x-ray (portable): used to determine
- Aortic dissection → wide mediastinum
- Pneumothorax → absence of lung markings
- Pulmonary edema → presence of fluid
Transthoracic ECHO (TTE) OR Transesophageal ECHO (TEE):
Useful in diagnosis of
- Myocardial infarction (MI) – wall motion abnormalities right ventricular (RV) infarction
- Cardiac structural abnormalities e.g. aneurysm, valvular sclerosis/stenosis, thrombi etc.
- Pericardial effusion
Stress test:
Assess coronary patency by myocardial uptake of radioactive dye (e.g. Technetium 99m Tc and Thallium-201).
Contrast computed tomography (CT) scan-chest: Used to differentiate STEMI from aortic dissection.
MRI with Gadolinium-rarely used: Enhancement of infarcted area and to differentiate STEMI from aortic dissection.
Considered after the initial management in patients with
- Evidence of ongoing ischemia (ECG findings or symptoms)
- Hemodynamic instability
- Recurrent ventricular tachyarrhythmia
[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”treatment-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Treatment
[/vc_column_text][cq_vc_tabs tabsstyle=”style2″ titlebg=”#16847d” titlehoverbg=”#333333″ rotatetabs=”0″][cq_vc_tab_item tabtitle=”Management & Therapies”]Goal: Minimize myocardial injury, preserve heart function and prevent complications.
Approach: Assess hemodynamic stability, implement emergency measures as required, determine treatment strategies and interventions to proceed.
1) ASSESSMENT FOR HEMODYNAMIC INSTABILITY
Often indicated by altered mental status, confusion, disorientation, severe hypotension, symptoms of shock and life-threatening arrhythmias.
2) EMERGENCY MEASURES
- ECG and continuous monitoring
- Pulse oximetry and blood pressure monitoring
- Oxygen inhalation
- Maintain IV and catheterize
- Monitor fluid intake/output
- Pain management
- Evaluation for reperfusion therapy
- Risk of thrombolytic therapy and contraindication for PCI
TREATMENT STRATEGIES FOR ACS
Treatment strategy is based upon risk group, i.e. low vs. high-risk patients, and predicts outcome according to TIMI risk score.
- TIMI risk score: Predicts outcome in patients with ACS
{kind=link}
A) TREATMENT STRATEGIES FOR UNSTABLE ANGINA AND NSTEMI

i) EARLY CONSERVATIVE STRATEGY (low-risk group)
- No history of recurrent attacks
- No evidence of myocardial injury
Treatment in the emergency room (ER):
Prompt attention in an ER for consideration of
OXYGEN inhalation
NITROGLYCERIN:
- Sublingual 0.3 to 0.4 mg, every 5 minutes up to 3 total dose
- For ongoing pain and/or hypertension, consider IV nitroglycerin
MORPHINE SULFATE:
- 2-4 mg IV slowly, with increments of 2-8 mg IV repeated at 5-15 minute intervals; maximum dose of 10 mg. Relieves pain, dyspnea, and anxiety
FENTANYL: (if allergic to morphine or hypotensive)
- 25-50 mcg IV (or intranasal)
BETA-BLOCKER:
Initiated orally in low and moderate doses within first 24 hrs, in patients who do not show the signs of low output state, heart failure, and heart block or have active asthma or reactive airway disease. Titrate according to heart rate and blood pressure.
IV metoprolol is of value in patients with ongoing ischemia with hypertension and who are not at risk of heart failure or cardiogenic shock.
Example
Metoprolol: Start within 24 hrs, if no contraindications exist.
- IV 5 mg every 2-10 mins up to a maximum dose of 15 mg
- Oral (low dose) 25 mg once daily; followed by 50 mg PO every 6 hrs for 48 hrs, and then 100 mg every 12 hrs, or as tolerated
CALCIUM CHANNEL BLOCKERS (CCBs):
Oral or IV administration of a non-dihydropyridine CCB (e.g. diltiazem and verapamil) may be used in hemodynamically stable patients with the ongoing acute coronary syndrome (ACS) in whom beta blockers are contraindicated.
Example: Diltiazem
- Immediate-release: Start 30 mg PO TID or BID; may increase 3 mg/dose every 1-2 days; usual 180-360 mg/day in divided doses; Max: 360 mg/day
- Extended-release: Initial 120-180 mg PO once daily, increase over 7-14 days; Max: 480 mg/day
STATIN
- Such as atorvastatin, rosuvastatin
ANTICOAGULANT
{kind=link}
Unfractionated heparin (UFH)
- Initial bolus of 60 U/kg (~4000-5000 U), then 12 U/kg/hr (~1000 U/hr) infusion should be administered promptly and adjusted to maintain aPTT ~1.5-2.0 times control
Low-molecular-weight heparin (LMWH)
- Enoxaparin: 1.0 mg/kg SC every 12 hrs; or use every 24 hrs if CrCl <30 mL/min
ANTIPLATELETS:
Acetylsalicylic acid (ASA): Typically 162 mg PO at presentation
- Followed by 81 to 325 mg daily
- If aspirin allergy or major intolerance, clopidogrel may be substituted
Clopidogrel:
- Administer 300 mg PO loading dose, followed by 75 mg daily. Used in conjunction with ASA or monotherapy for those intolerant to ASA
Dual antiplatelet therapy:
ASA plus Clopidogrel or Ticagrelor: Usually for 1 year in all acute coronary syndrome (ACS) patients including those requiring PCI and/or CABG unless known specific contraindication; followed by monotherapy.
- ASA (81 mg ) plus Clopidogrel (75 mg)
ii) EARLY INVASIVE STRATEGY (high risk group)
- Recurrent ischemia on medical management
- Evidence of myocardial injury
- Congestive heart failure
- Left ventricular dysfunction
- Sustained ventricular tachycardia
- Prior coronary revascularization
- PCI within 6 months
- Coronary artery bypass grafting (CABG)
Medical Management
Nitroglycerin, opiates, beta blockers, CCBs, statins are used as shown above
➢ Anticoagulant
➢ Antiplatelet
➢ Intervention strategie
ANTICOAGULANT
Heparin/LMWH:
- As used above
Fondaparinux:
- 2.5 mg SC once daily; up to 8 days or until hospital discharge
Bivalirudin:
Always given with ASA or clopidogrel
- Angiography: Initial IV bolus of 0.1 mg/kg followed by an infusion of 0.25 mg/kg/h prior to angiography and continued through angiography and as required
- PCI: Give additional bolus of 0.5 mg/kg and increase infusion to 1.75 mg/kg, then reduce infusion to 0.25 mg/kg/h following post PCI
Argatroban:
- Bolus 350 mcg/kg IV over 3-5 minutes and start 25 mcg/kg/minute IV infusion; check activated clotting time (ACT) after 5-10 minutes of bolus infusion and titrate to keep ACT 300-450
ANTIPLATELETS:
Aspirin:
Typically 162 mg PO at presentation
- Followed by 81 to 325 mg daily
- If aspirin allergy or major intolerance, clopidogrel may be substituted
Clopidogrel:
- Administer 300 mg PO loading dose, followed by 75 mg daily. Used as monotherapy if ASA intolerance, but most often as dual therapy
Dual antiplatelet therapy:
Is often given for 1 year in all acute coronary syndrome (ACS) patients including those requiring PCI and/or coronary artery bypass graft (CABG) unless known to specific contraindication; followed by monotherapy.
ASA plus Clopidogrel:
- 300 mg PO loading dose, followed by 75 mg/day plus ASA (81 mg)
- For at least 1 month in patients who receive BMS (bare-metal stent)
- For at least 1 year in patients who receive DES (drug-eluting stent)
ASA plus Ticagrelor:
- Initial single loading dose of 180 mg PO then 90 mg every 12 hrs plus ASA 75 to 150 mg once daily for 1 year unless contraindicated
ASA plus Prasugrel:
- Acute coronary syndrome (ACS) managed with PCI. Initial 60 mg PO loading dose; usual 10 mg PO at bed time plus ASA 75-325 mg/day for ~1 year
- Note: Contraindicated in patients with prior stroke or TIA; and has a relative contraindication in patients with age >75 years or weight less than 60 kg
GLYCOPROTEIN IIb/IIIa INHIBITORS (optional use as decided by the cardiologist)
Used in combination with ASA and heparin.
Eptifibatide or Tirofiban: Maybe considered in all acute coronary syndrome (ACS) including those with PCI.
Abciximab: Considered in ACS requiring PCI.
Abciximab:
- 0.25 mg/kg IV bolus 10-60 min prior to start of PCI; Max. 10 mcg/min; followed by an infusion of 0.125 mcg/kg/min for 12 hr
Eptifibatide:
- 180 mcg/kg IV bolus just prior to PCI, followed by continuous infusion of 2 mcg/kg/min (max. of 15 mg/hr). Second bolus of 180 mcg/kg given 10 minutes after initial bolus. Infusion should be continued for up to 18-24 hrs
Tirofiban:
- 25 mcg/kg IV over 3 minutes at the time of PCI; 0.15 mcg/kg/min infusion continues for up to 18-24 hr
Interventions and Surgeries
- Diagnostic angiography
- Primary percutaneous coronary intervention (PCI)
- Early reperfusion therapy reduces the infarct size and increases survival
- Coronary artery bypass graft (CABG)
B) TREATMENT STRATEGY FOR STEMI
Once a patient meets the diagnostic criteria for STEMI treatment includes:
General measures
- BP monitoring and pulse oximetry
- Supplemental O2
- Two peripheral IV lines
- Foley catheter
- Continuous cardiac monitoring
Medical management
- Nitroglycerin, opiates, beta blockers, statins, anticoagulant, antiplatelet therapy are used as shown above
Interventions and Surgeries
1) Diagnostic angiography
2) Coronary reperfusion therapy
a) Primary percutaneous coronary intervention (PCI)
- More effective than fibrinolytic therapy; the latter is only indicated when PCI is not available or being delayed
- Early reperfusion therapy reduces the infarct size and increases survival
b) Fibrinolytic therapy
If PCI not an option/available.
Fibrin selective agents:
- Tissue plasminogen activator (tPA)-Alteplase: 15 mg IV bolus 0.75 mg/kg over 30 min then 0.5 mg/kg over 60 min IV
- Recombinant plasminogen activator(r-PA)-Reteplase: 10 Unit IV bolus over 2 mins given 30 min apart; hold second dose if life-threatening bleeding or anaphylactic reaction occurs
- TNK-tPA-Tenecteplase: Single IV bolus: 30 mg if <60 kg; 35 mg if 60-70 kg; 40 mg if 70-80 kg; 45 mg if 80-90 kg; 50 mg if >90 kg body weight
Fibrin non-selective agents:
- Streptokinase: 1.5 million Units over 30-60 min IV
3) Coronary artery bypass graft (CABG)
Emergency CABG
Approximately 10% of acute coronary syndrome (ACS) patients requires CABG during the index admission
Indications
- Severe left main artery disease
- Refractory ischemia
- Failed PCI
- Multivessel disease with reduced left ventricular ejection fraction
- Cardiogenic shock
Bleeding Risk:
- The use of combined ASA plus clopidogrel prior to CABG is assessed by risk of early fatal event vs. risk of major bleeding. If the risk of the former outweighs the latter then the surgery is conducted with dual therapy (such as refractory ischemia despite optimal medical treatment, and those with high-risk coronary anatomy e.g. severe left main stenosis with severe right coronary artery disease). However, if risk of bleed outweighs recurrent fatal event then hold clopidogrel for 3-5 days prior to CABG
Ref: Fitchett et al. Can J Cardiol 2009:25(12):683-689.
C) POST MI MEDICAL THERAPY-TREATMENT OPTIONS
Nitroglycerin
- As indicated for recurrent chest pain
Beta-blockers:
- In general, are used to help control angina and improve survival in patients with prior MI and heart failure due to systolic dysfunction
ACE inhibitors:
- Reduces short term mortality, and is beneficial in patients with EF<40%
- Administration within 24 hours reduce the incidence of CHF and recurrent MI
- Contraindicated in hypotension, hyperkalemia, acute kidney failure, renal stenosis
Angiotensin II receptor blockers (ARBs):
- Benefits similar to ACEIs in acute coronary syndrome
- Can be used in ACEIs intolerant patients
- Combination ARB plus ACEI: Limited value in select patients
Aldosterone receptor antagonists: (e.g. spironolactone)
Beneficial in:
- Post MI patients with LV ejection fraction of ≤40%
- Symptomatic heart failure
- DM without significant renal dysfunction
Requires caution in hyperkalemia and renal insufficiency
Statins:
- Initiated during hospitalization for ACS
- Continued use is recommended in patients incurring MI while on statin therapy
- Goal is at least 50% reduction in LDL or LDL <2.0 mmol/L (70 mg/dL)
- Dyslipidemia targets
{kind=link}
Antiplatelet therapy: For prevention of recurrent thrombosis
- ASA plus Clopidogrel/Ticagrelor/Prasugrel – used for 1 year as discussed above and then followed by monotherapy (usually ASA indefinitely)
Anticoagulant therapy: For cardioembolic prophylaxis
- Warfarin (INR 2-3): Indicated in large anterior wall MI for 3 months or presence of AF
- Dabigatran: Consider if AF present and creatinine clearance (CrCl) >30 mL/min
- Age <80 year: 150 mg PO BID
- Age >80 year: 110 mg PO BID
- Rivaroxaban: Consider if AF present
- 20 mg PO once daily if CrCl ≥50 mL/min
- 15 mg PO once daily if CrCl 30-49 mL/min
- Apixaban: Consider if AF present
- GFR >25 ml/min: 5 mg PO BID
- Alternatively, 2.5 mg BID may be considered in patients with at least 2 of: Age ≥80 years, body weight ≤60 kg, or serum creatinine ≥133 micromole/L (1.5 mg/dL)
D) POST MI RISK ASSESSMENT
Indicated for patients:
- Presenting >24 hours after symptoms
- Who received thrombolytic therapy
- Receiving medical therapy alone
Assessments:
- TIMI risk score
- GRACE score
- Stress testing
- Cardiac catheterization
- In high-risk individuals
{kind=link}
{kind=link}
{kind=link}
E) COMPLICATIONS FOLLOWING ACUTE MI
1) Recurrent chest pain:
- Re-evaluate from recurrent MI
2) Acute pericarditis:
- Pleuritic pain
- – Typically occurs within 1-4 days post-MI
- – Relieved in an upright position
3) Dressler syndrome:
- Malaise, fever, chest pain
- Autoimmune-mediated
- Typically occurs 1-8 weeks after MI
- Laboratory
- – Leukocytosis/ high ESR
- – Echocardiogram (ECHO)-pericardial effusion
4) Arrhythmias:
- Palpitations, lightheadedness, syncope
- Send for coagulation profile along with other labs
- ECG/telemetry
5) Cardiogenic shock:
- Hypotension, shortness of breath (SOB), pallor, diaphoresis, cold clammy skin, and weak pulses
- Requires urgent attention
6) Stroke:
- Abrupt onset of neurological disturbance, e.g. hemiparesis, loss of speech or vision
- If symptoms persist it is defined as “Stroke”
- If symptoms are a transient suspect transient ischemic attack (TIA)
- Rule out ischemic vs. hemorrhagic insult supported by further workup and investigations
- CT brain
- Carotid doppler/ computed tomography angiography (CTA)/ magnetic resonance angiography (MRA)
- ECG/telemetry
- Echocardiogram (ECHO)
Mechanical and structural complications following acute myocardial infarction (MI)
- Left ventricular aneurysm
- Ventricular pseudoaneurysm
- Papillary muscle rupture
- Ventricular septal rupture
- Treatment:
- Stabilize patient hemodynamically
- Surgical repair
[/cq_vc_tab_item][cq_vc_tab_item tabtitle=”Medication Dose”]MEDICATIONS
{kind=link}
- Aspirin
- Clopidogrel
- Prasugrel
- Ticagrelor
- Glycoprotein IIb/IIIa inhibitors (GPIIb/IIIa inhibitors)
Mechanisms:
Aspirin
- Works through cyclooxygenase pathway (COX 1-2 )
- Inhibits platelet aggregation
- Antipyretic, anti-inflammatory and analgesic action
- Antiplatelet effects last ~7-10 days
Clopidogrel/ Prasugrel
- Binds to adenosine diphosphate (ADP) → impairs activation of receptor complex → inhibits platelet aggregation
- Antiplatelet effects last ~7-10 days
Ticagrelor
- Selective and reversibly bound antagonists of the adenosine diphosphate (ADP) P2Y12 receptor
- Ticagrelor acts on platelet P2Y12 receptors and prevents ADP-mediated platelet activation and aggregation, by interacting with a binding site different from that of ADP (non-competitive antagonism)
GPIIb/IIIa inhibitors
- Selectively binds to the glycoprotein IIb/IIIa (GPIIb/IIIa) receptor on the surface of platelets
- Prevents binding of fibrinogen, von Willebrand factor, and other adhesive molecules to GPIIb/IIIa receptor sites on activated platelets
- Decrease platelet aggregation and prevents thrombosis
Dose:
Aspirin
Acute coronary syndrome
- 162-325 mg PO once daily
MI prevention/ Vascular prophylaxis
- 75-325 mg PO daily
Clopidogrel
Unstable angina, MI
- Loading dose 300 mg, followed by 75 mg PO daily; in combination with aspirin 75-325 mg initially, then 75-162 mg/day
Percutaneous coronary intervention (PCI)
- Loading dose 300-600 mg given as early as possible before or at the time of PCI followed by 75 mg PO once daily
Recent MI/ Recent stroke/ Peripheral arterial disease (PAD)
- Oral: 75 mg PO once daily
Prasugrel
Acute coronary syndrome managed with PCI:
- Initial 60 mg PO loading dose; usual 10 mg PO at bedtime with Aspirin 75-325 mg/day
Ticagrelor
- Initial single 180 mg PO loading dose; then 90 mg PO every 12 hrs
- Note: Ticagrelor should be taken with acetylsalicylic acid (ASA) between 75 mg and 150 mg PO once daily, unless specifically contraindicated.
Switching from Clopidogrel to Ticagrelor:
- Administer the first 90 mg dose of Ticagrelor 24 hours following the last dose of Clopidogrel
{kind=link}
- Unstable angina refractory to medical therapy
- Percutaneous coronary intervention (PCI)
{kind=link}
- Acute coronary syndrome / PCI ± stent
- Dose in renal impairment
{kind=link}
- UA/NSTEMI
- STEMI + PCI
- Dose in renal impairment
{kind=link}
- Nitroglycerin
- Isosorbide dinitrate
- Isosorbide mononitrate
Mechanisms:
Stimulates intracellular cyclic-GMP, results in
- Vascular smooth muscle relaxation and peripheral vasodilatation
- Decrease pre and after-load thus reduces myocardial oxygen demand
- Nitroglycerin dilates coronary arteries
Dose:
{kind=link}
- Acute angina
- Angina prophylaxis
- Acute MI
Isosorbide dinitrate
Acute angina/Prophylactic management
- Sublingual: 2.5-5 mg every 5-10 minutes for a maximum of 3 doses in 15-30 minutes
Long-term angina-prophylaxis
- 5-20 mg PO BID-TID, followed by maintenance dosage of 10-40 mg BID-TID
- Extended-release tabs: 40-80 mg PO every 8-12 hrs
Isosorbide mononitrate
Angina
- 5-20 mg PO BID; Max. 40 mg/day
- Titration: Increase to 10 mg PO BID in first 2-3 days
- Extended-release tablet: 30-60 mg PO every morning; Max. 240 mg/day
- Titration: Increase as required, with at least 3 day interval
{kind=link}
- Morphine
- Fentanyl
Mechanism:
Binds to opiate receptors at many sites within the CNS, causes
- Increases pain threshold-inhibits ascending pain pathway
- Alter perception of and emotional response to pain
- Generalized CNS depression
Dose:
Morphine
- 2-4 mg IV slowly, with increments of 2-8 mg IV repeated at 5-15 minutes intervals; maximum dose of 10 mg. Relieves pain, dyspnea, and anxiety
Fentanyl
- 50-100 mcg/dose IV/IM every 1-2 hrs as required
{kind=link}
- Injectable
- Heparin
- Enoxaparin (LMWH)
- Dalteparin (LMWH)
- Fondaparinux
- Bivalirudin
- Argatroban
- Oral
- Warfarin
- Dabigatran
- Rivaroxaban
- Apixaban
Mechanisms:
- Inhibits thrombus formation
- May prevent propagation of existing thrombi
- No direct lytic effect on established thrombi
- Prolongs aPTT
Doses:
{kind=link}
- PCI ± concurrent GPIIb/IIIa inhibitor
- STEMI: Adjunct therapy
- UA/NSTEMI
{kind=link}
{kind=link}
- STEMI
- UA/NSTEMI
- PCI adjunct therapy
Dalteparin (LMWH)
UA / NSTEMI
- 120 IU/kg body weight SC every 12 hrs for 5-8 days with simultaneous aspirin; Max. 10,000 IU/dose
- Discontinue once patient is clinically stable
Fondaparinux (factor Xa inhibitor)
STEMI
- 2.5 mg IV stat; Then 2.5 mg SC once daily for up to 8 days or until hospital discharge
UA / NSTEMI
- Administer 2.5 mg SC once daily for up to 8 days or until hospital discharge
- Renal impairment: Contraindicated if CrCl <30 mL/minute
{kind=link}
Should be administered with ASA, concomitantly Clopidogrel can also be administered
- UA/ NSTEMI
- Percutaneous coronary intervention (PCI)
- Subsequent to heparin (UFH/LMWH)
{kind=link}
- Percutaneous coronary intervention (PCI)
- Post PCI
- Dose in hepatic impairment
Warfarin
Prevention/Treatment of thrombosis/Embolism
- Start 2-10 mg PO once daily for 1-2 days then adjust dose according to INR results
- Desired INR 2-3 for non-mechanical valves. Maybe acceptable for aortic bileaflet mechanical valve without thromboembolism risk factors
- OR
- INR 2.5-3.5, if the concomitant mitral mechanical valve or aortic mechanical valve
Ref: Bonow Ro, Carabello BA, Chatterjee K et al. Circulation. 2008; 118: e523-e661.
Warfarin dosing – Suggested protocol in adults (no mechanical valve)
{kind=link}
Warfarin dosing – Suggested protocol in adults (with mechanical valve)
{kind=link}
Warfarin reversal – Suggested protocol
{kind=link}
Dabigatran
Dosage (Canada):
- Age <80 year: 150 mg BID if creatinine clearance >30 mL/min
- Age >80 years: 110 mg BID if creatinine clearance >30 mL/min
- Contraindicated in creatinine clearance <30 mL/min
Conversion from Dabigatran to parenteral anticoagulant
- Wait 12 hrs after the last dose of Dabigatran before switching to a parenteral anticoagulant
Conversion from Vitamin K antagonists (e.g. warfarin) to Dabigatran
- Dabigatran should only be started after Vitamin K antagonists have been discontinued, and the patient’s INR found to be <2.0
Conversion from Dabigatran to Vitamin K antagonists (e.g. warfarin)
- Stop Dabigatran for 12 hrs then begin Warfarin protocol/nomogram (see above)
Rivaroxaban
Nonvalvular atrial fibrillation:
- 20 mg PO once daily for CrCl >50
- 15 mg PO once daily for CrCl 30-49
Apixaban
Nonvalvular atrial fibrillation:
- GFR >25 ml/min: 5 mg PO BID
- Alternatively, 2.5 mg BID may be considered in patients with at least 2 of the following:
- Age ≥80 years
- Body weight ≤60 kg
- Serum creatinine ≥133 micromole/L (1.5 mg/dL)
Beta-adrenergic blocking agents:
{kind=link}
- Cardioselective:
- Acebutolol
- Atenolol
- Metoprolol
- Non-Cardioselective:
- Carvedilol
- Nadolol
- Propranolol
- Timolol
Mechanism:
- Block beta receptors
- Decreases heart rate and cardiac output
- Decreases renin release (more efficacious in populations with elevated plasma renin activity such as younger white patients)
Dose:
Cardioselective:
Acebutolol
Angina / Ventricular arrhythmia
- 400 mg/day PO in divided doses; usual 600-1200 mg/day in divided doses Max.1200 mg/day
Atenolol
Post-myocardial infarction
- 50 mg/day PO daily or BID or 100 mg daily (as tolerated)
Metoprolol
Angina
- Immediate-release: Start 25 mg PO BID; maintenance 50-200 mg PO BID; Max. 400 mg/day; begin with low dose and increase dose at weekly intervals to the desired effect
- Extended-release: Initial 100 mg/day; Max. 400 mg/day
Myocardial infarction (acute)
- Initial 5 mg IV every 2 mins for 3 doses then 50 mg PO every 6 hrs x 48 hrs starts 15 minutes after last IV dose; maintenance dose 100 mg PO BID
- Note: If initial IV dose is not tolerated then give 25-50 mg PO every 6 hrs
- Secondary prevention: Immediate release (IR) 25-100 mg PO BID; optimize dose based on heart rate and blood pressure; continue indefinitely
Non-Cardioselective:
Carvedilol
LV dysfunction following MI
- Immediate-release: Initial 3.125-6.25 mg PO BID; increase dosage at intervals every 3-10 days; may increase to 25 mg PO BID if required
- Extended-release (available in the USA only): Initial 10-20 mg/day PO daily; increase dosage at intervals every 3-10 days; target dose of 80 mg/day PO daily as tolerated
Nadolol
Angina / Hypertension
- Initial 40 mg/day daily; typically 40-80 mg/day daily; Max. 320 mg/day daily
- Titration: Gradually increase every 3-7 days until optimum clinical response is obtained or maximum dose achieved
Propranolol
Post-MI
- 60-80 mg/day PO TID as tolerated; may increase to 180-240 mg/day (divided doses)
Timolol
Myocardial infarction, secondary prevention
- Start 10 mg PO BID within 4 weeks of MI
Angina
- Initial 10 mg PO BID; range 10-60 mg/day PO divided BID-TID
ACE (angiotensin-converting enzyme) inhibitors:
{kind=link}
- Captopril
- Enalapril
- Lisinopril
- Perindopril
- Ramipril
- Trandolapril
Mechanisms:
- Inhibits renin-angiotensin aldosterone system and bradykinin degradation
- Stimulate vasodilating prostaglandin synthesis
- Reduce sympathetic nervous system activity
- Relatively less effective in those of African descent and in the elderly
Dose:
Captopril
LV dysfunction following MI
- Start 6.25 mg PO daily; followed by 12.5 mg PO QID
- Titration: Increase to 25 mg PO TID over every 3-7 days; followed by gradual increase over weeks to 50 mg PO TID as tolerated
Enalapril
Acute MI
- Initial 2.5 mg PO daily within 48h post-MI, quickly titrate dose up; usual 10 mg PO QID
Lisinopril
Acute MI
- 5 mg PO immediately, then 5 mg at 24 hours, 10 mg at 48 hours, and 10 PO daily for 6 weeks
Perindopril
Coronary artery disease
- Initial 4 mg PO daily for 2 weeks; then increase as tolerated to 8 mg PO daily
Ramipril
LV dysfunction following MI
- Start 2.5 mg PO BID; then increase every 3 weeks if possible to target of 5 mg PO BID
Cardiovascular event prevention
- Start 2.5 mg PO daily for 1 week; then increase as tolerated to 10 mg once daily or BID
Trandolapril
Post-MI heart failure or LV dysfunction
- Initial 1 mg/day PO daily; Max. 4 mg/day; then increase as tolerated to 4 mg/day
Angiotensin receptor blocking agents (ARB):
{kind=link}
- Telmisartan
- Irbesartan
- Losartan
- Valsartan
Mechanisms:
- Block AT1 angiotensin receptors
- Blocks the vasoconstrictor and aldosterone secreting effect of angiotensin II
- Reduce vasoconstriction
Dose:
Telmisartan
Cardiovascular risk reduction
- Initial 80 mg PO daily
Valsartan
Left ventricular dysfunction after MI
- 20 mg PO BID; Max. 160 mg
- Titration: Increase dose to target of 160 mg BID as tolerated
Irbesartan
Cardiovascular risk reduction/ Hypertension
- Initial 150 mg PO daily; may increase to 300 mg daily; Max. 300 mg
Losartan
Cardiovascular risk reduction/ Hypertension
- 50 mg PO daily; Max. 100 mg
Aldosterone receptor blockers:
{kind=link}
- Spironolactone
- Eplerenone
Mechanism:
- Block aldosterone receptors in renal collecting tubule → results in increased excretion of sodium and water and decreased excretion of potassium
- Spironolactone is often co-administered with thiazide or loop diuretics in the treatment of edema and hypertension
Dose:
Spironolactone
Heart failure, severe (NYHA-class III/IV)
- 12.5-25 mg/day; Max. 50 mg/day
- Titration: Increase to 50 mg/day after 8 weeks or as tolerated in worsening CHF
Edema
- 25-200 mg/day PO once daily or in two divided doses
Eplerenone
Heart failure (post-MI)
- Initial 25 mg PO daily
- Titration: Increase to 50 mg daily within 4 weeks, or as tolerated
- Note: Adjust the dose as per serum potassium concentrations
Calcium channel blocking agents (CCBs):
{kind=link}
- Diltiazem
- Verapamil
Mechanisms:
- Blocks the inward movement of calcium by binding to the L-type calcium channels in the heart and in smooth muscle of the peripheral vasculature
- This decreases intracellular calcium leading to a reduction in muscle contraction
- Significantly reduces afterload, with no effect on preload
Dose:
Non-Dihydropyridines
Diltiazem
Angina
- Immediate-release: Start 30 mg PO TID or QID; may increase 30mg/dose every 1-2 days; usual 180-360 mg/day BID; Max. 360 mg/day
- 24h extended-release: Initial 120-180 mg PO daily, increase over 7-14 days; Max. 480 mg/day
Verapamil
Angina
- Immediate-release: Initial 80-120 mg PO QID; usual range 80-160 mg PO QID
- Elderly or small stature: 40 mg 3 times/day
- 24h extended-release: 180 mg PO daily; Max. dose 480 mg/day
- If inadequate response, may increase dose at weekly intervals to 240 mg/day PO, then 360 mg/day, then 480 mg/day if required and as tolerated
Statins (HMG-CoA reductase inhibitor):
{kind=link}
- Atorvastatin
- Simvastatin
- Fluvastatin
- Lovastatin
- Pravastatin
- Rosuvastatin
Mechanism:
- Inhibits 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase
- This reduces the conversion of mevalonic acid from HMG-CoA
- An early precursor of cholesterol
- This results in compensatory increase in the number of low-density lipoprotein (LDL) receptors on hepatocyte membranes
- This stimulates LDL catabolism and leads to reduction in LDL production
Dose:
Atorvastatin
- Start 40-80 mg PO daily; adjust dose based on patient’s tolerability and recommended LDL-C goal
Simvastatin
- 40 mg PO daily at bedtime; usual range 10-40 mg/day
- Do not exceed 20 mg/day if given concomitantly with amiodarone or verapamil
- Do not exceed 40 mg/day if given concomitantly with diltiazem
- CrCl <10 mL/minute: Start 5 mg/day with close monitoring
Fluvastatin
- 40 mg PO daily at bedtime; may increase to 80 mg/day PO once daily or in 2 divided doses
Lovastatin
- Start 20 mg PO daily at bedtime; may increase to 40 mg PO daily at bedtime after at least 4 week interval
Pravastatin
- Start 40 mg PO daily at bedtime; may increase up to 80 mg PO to achieve desired effect, after at least every 4 week. Starting dose in renal impairment is 10 mg PO at bedtime
Rosuvastatin
- Start 5-10 mg PO daily at bed time; may increase every 2-4 weeks; usual dose 20 mg/day
{kind=link}
- Fibrin selective agents:
- Alteplase (tPA)
- Reteplase (r-PA)
- Tenecteplase (TNK-tPA)
- Fibrin non-selective agents:
- Streptokinase
- Urokinase (uPA)
Mechanisms:
- These agents stimulates plasminogen activator → forms a complex by binding with fibrin and plasminogen
- This complex → converts residual plasminogen into plasmin, a proteolytic enzyme capable of hydrolyzing fibrin
- Unopposed plasmin digests fibrinogen and other plasma proteins, including factors V and VIII
Dose:
Alteplase (tPA)
In ST-elevation MI (STEMI)
{kind=link}
Reteplase (r-PA)
ST-elevation MI (STEMI) / Pulmonary embolism (PE)
- 10 IU IV over 2 minutes; then repeat 30 mins later
- Hold the second dose if serious bleeding or anaphylaxis occurs
Tenecteplase (TNK-tPA)
ST-elevation myocardial infarction (STEMI)
{kind=link}
Streptokinase
Acute evolving transmural myocardial infarction
- IV infusion: Usual dose 1.5 million IU over 60 minutes
- Intracoronary infusion: 20,000 IU bolus, then 2000 IU/min for 1 hrs; total dose 140,000 IU
Urokinase (uPA)
Coronary artery thrombosis and Acute MI
- 2-3 million IU IV over 45-90 minutes
- Give 50% or 100% of the dose as IV bolus (e.g. over 5 minutes); remainder, if any, as a continuous infusion
- Administer concurrently with heparin
[/cq_vc_tab_item][/cq_vc_tabs][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”clinical-trials-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Clinical Trials
[/vc_column_text][vc_column_text]
- OASIS-6–Effects of Fondaparinux on Mortality and Reinfarction in Patients With Acute ST-Segment Elevation Myocardial Infarction
- CURE trial–Effects of Clopidogrel in Addition to Aspirin in Patients with Acute Coronary Syndromes without ST-Segment Elevation
- PLATO–Ticagrelor versus Clopidogrel in Patients with Acute Coronary Syndromes
- Re-LY–Dabigatran versus Warfarin in Patients with Atrial Fibrillation
- ROCKET AF– Rivaroxaban versus Warfarin in Nonvalvular Atrial Fibrillation
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”pipe-line-agents-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Pipeline Agents
[/vc_column_text][vc_column_text]
- TRACER study-Thrombin-Receptor Antagonist Vorapaxar in Acute Coronary Syndromes
- TIMACS study-Early versus Delayed Invasive Intervention in Acute Coronary Syndromes
{kind=link}
{kind=link}
[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”physician-resources-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
Physician Resources
[/vc_column_text][vc_column_text]1. Tips for Patient Care
Risk factor management:
Patients with CAD have a high risk of recurrent MI and stroke
- Advise patient on how to respond to recurrent chest pain with SL nitroglycerin
- Emphasize on risk factor management (HTN, DM, obesity etc.)
- Reinforce early smoking cessation
- Compliance with medications
Medications:
- Advise patient to establish a daily routine for pill-taking
- Simplify the medication regimen to improve compliance
- Consider the use of combination pills
- Consider concurrent risk factors and disease states with the prescribed therapy
- In elderly patients consider lower starting doses to avoid side effects
- Hormone replacement therapy is not indicated for primary or secondary prevention of cardiovascular events in postmenopausal women
Social and Stress factors:
- Include family or social support in lifestyle modification
- Be aware that reactive depression may occur
Physical activity:
- Gradually increase physical activity during the first 3 to 6 wk post discharge
- Many patients can return to all their normal activities if good cardiac function is maintained ~6 wks after post-MI
2. Scales and Tables
{kind=link}
{kind=link}
[/vc_column_text][/vc_column_inner][/vc_row_inner][vc_row_inner column_margin=”default” text_align=”left” el_id=”references-title”][vc_column_inner column_padding=”no-extra-padding” column_padding_position=”all” background_color_opacity=”1″ background_hover_color_opacity=”1″ column_shadow=”none” column_border_radius=”none” column_link_target=”_self” width=”1/1″ tablet_width_inherit=”default” column_border_width=”none” column_border_style=”solid” bg_image_animation=”none”][vc_column_text]
References
[/vc_column_text][vc_column_text]Core Resources:
- Antman EM, Cohen, M, Bernink, PJ, et al. The TIMI risk score for unstable angina/non-ST elevation MI: A method for prognostication and therapeutic decision-making. JAMA. 2000; 284:835-842
- Bell AD, Roussin A, Cartier R. et al. The Use of antiplatelet therapy in the out-patient setting: Canadian Cardiovascular Society Guidelines. Can J Cardiol. 2011;27: S1-S59
- Compendium of Pharmaceuticals and Specialties (CPS). Canadian Pharmacist Association. Toronto: Webcom Inc. 2012
- Day RA, Paul P, Williams B, et al (eds). Brunner & Suddarth’s Textbook of Canadian Medical-Surgical Nursing. 2nd ed. Philadelphia: Lippincott Williams and Wilkins; 2010
- Fitchett D, Eikelboom J, Fremes S, et al. Dual antiplatelet therapy in patients requiring urgent coronary artery bypass grafting surgery: A position statement of the Canadian Cardiovascular Society. Can J Cardiol 2009;25(12):683-689
- Foster C, Mistry NF, Peddi PF, Sharma S, eds. The Washington Manual of Medical Therapeutics. 33rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2010
- Gonçalves PD, Ferreira J, Aguiar C, Seabra-Gomes R. TIMI, PURSUIT, and GRACE risk scores: sustained prognostic value and interaction with revascularization in NSTE‐ACS. Eur Heart J (May 2005) 26 (9): 865-872
- DOI: 10.1093/eurheartj/ehi187
- Genest J, McPherson R, Frohlich J, et al. Canadian Cardiovascular Society/Canadian guidelines for the diagnosis and treatment of dyslipidemia and prevention of cardiovascular disease in the adult-2009 recommendations. Can J Cardiol. 2009; 13(10):567-579
- DOI: 10.1016/S0828-282X(09)70715-9
- Gray J, ed. Therapeutic Choices. Canadian Pharmacists Association. 6th ed. Toronto: Webcom Inc. 2011
- Hess EP, Agarwal D, Chandra S, et al. Diagnostic accuracy of the TIMI risk score in patients with chest pain in the emergency department: a meta-analysis. CMAJ. 2010; 182:1039-1044
- DOI: 10.1503/cmaj.092119
- JG Howlett, RS McKelvie, J Costigan, et al. The 2010 Canadian Cardiovascular Society guidelines for the diagnosis and management of heart failure update: Heart failure in ethnic minority populations, heart failure and pregnancy, disease management, and quality improvement/assurance programs. Can J Cardiol 2010;26(4):185-202
- Katzung BG, Masters SB, Trevor AJ, eds. Basic and Clinical Pharmacology. 11th ed. New York: McGraw-Hill; 2009
- Longo D, Fauci A, Kasper D, et al (eds). Harrison’s Principles of Internal Medicine. 18thed. New York: McGraw-Hill; 2011
- McPhee SJ, Papadakis MA, eds. Current Medical Diagnosis & Treatment. 49th ed. New York: McGraw-Hill; 2010
- Nova Scotia Guidelines for Acute Coronary Syndromes. Halifax, NS: Cardiovascular Health Nova Scotia; 2008
- O’Rourke R, Walsh R, Fuster V, eds. Hurst’s the Heart Manual of Cardiology, 12thEdition. New York: McGraw-Hill; 2008
- Pagana KD, Pagana TJ eds. Mosby’s Diagnostic and Laboratory Test Reference. 9th ed. St. Louis: Elsevier-Mosby; 2009
- Skidmore-Roth L. ed. Mosby’s drug guide for nurses. 9th ed. St. Louis: Elsevier-Mosby; 2011
- Skidmore-Roth L, ed. Mosby’s nursing drug reference. 24th ed. St. Louis: Elsevier-Mosby; 2011
Online Pharmacological Resources:
- e-Therapeutics
- Lexicomp
- RxList
- Epocrates
- Cardiovascular Health Nova Scotia
- Health Canada
Journals/Clinical Trials:
- Anderson HV, Cannon CP, Stone PH et al. One-year results of the Thrombolysis in Myocardial Infarction (TIMI) IIIB clinical trial. A randomized comparison of tissue-type plasminogen activator versus placebo and early invasive versus early conservative strategies in unstable angina and non-Q wave myocardial infarction. J Am Coll Cardiol. 1995;26(7):1643-1650
- Arnold JM, Yusuf S, Young J, et al. Prevention of Heart Failure in Patients in the Heart Outcomes Prevention Evaluation (HOPE) Study. Circulation. 2003; 107: 1284-1290
- Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med 2009;361:1139-1151
- Fox KM. Efficacy of perindopril in reduction of cardiovascular events among patients with stable coronary artery disease: randomised, double-blind, placebo-controlled, multicentre trial (the EUROPA study). Lancet. 2003; 362(9386):782-8
- Morrow DA, Scirica BM, Fox KA, et al. Evaluation of a novel antiplatelet agent for secondary prevention in patients with a history of atherosclerotic disease: design and rationale for the Thrombin-Receptor Antagonist in Secondary Prevention of Atherothrombotic Ischemic Events (TRA 2 degrees P)-TIMI 50 trial. Am Heart J. 2009; 158(3):335-41
- Patel M, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med 2011; 365:883-891
- DOI: 10.1056/NEJMoa1009638
- Wallentin L, Becker RC, Budaj A, et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N Engl J Med 2009; 361:1045-1057
- DOI: 10.1056/NEJMoa0904327
- Yusuf S, Zhao F, Mehta SR, et al. Effects of Clopidogrel in Addition to Aspirin in Patients with Acute Coronary Syndromes without ST-Segment Elevation. N Engl J Med 2001; 345:494-502
- Yusuf S, Mehta SR, Chrolavicius S, et al. Effects of fondaparinux on mortality and reinfarction in patients with acute ST-segment elevation myocardial infarction: the OASIS-6 randomized trial. JAMA. 2006;295(13):1519-30
[/vc_column_text][/vc_column_inner][/vc_row_inner][/vc_column][/vc_row]