Ischemic Stroke
ACKNOWLEDGEMENTS:
Thanks to Dr Andre G. Douen, MD, PhD, FRCPC, FAHA, Consultant Neurologist, Former Division Head, Neurology, Trillium Health Partners, Mississauga, ON Canada for his expertise with the initial review of this topic.
[pdf-embedder url=”https://www.educateyourhealth.com/wp-content/uploads/2019/04/Stroke-Brochure.pdf” width=”750″]
Definition
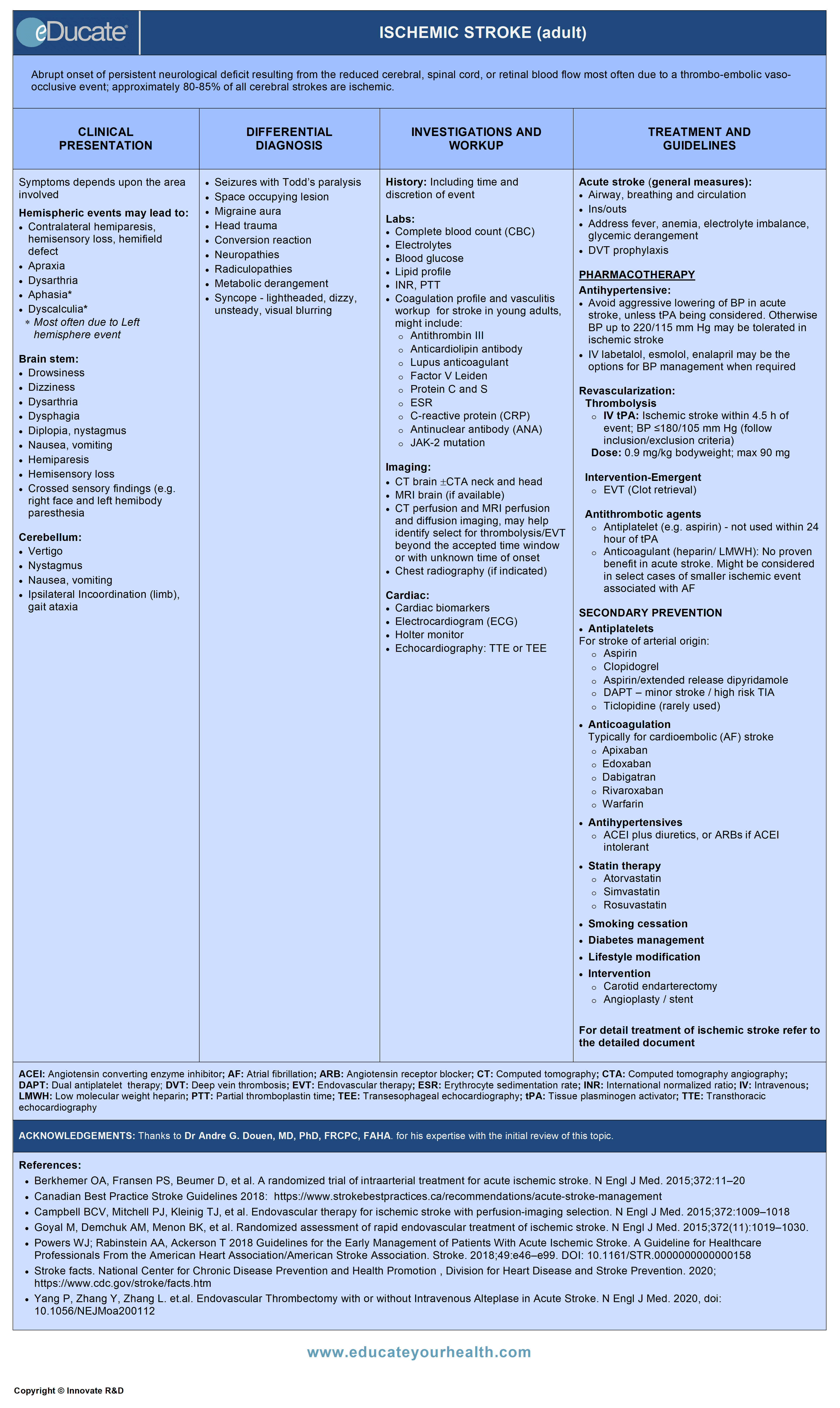
Abrupt onset of persistent neurological deficit resulting from the reduced cerebral, spinal cord, or retinal blood flow most often due to a thrombo-embolic vaso-occlusive event; approximately 80-85% of all cerebral strokes are ischemic.
Etiology
Cerebral Acute Ischemic Stroke (AIS):
Approximately 80-85% involves the anterior circulation (carotids and associated intracranial vessels), ~15-20% involve the posterior circulation (vertebrobasilar and posterior cerebral arteries).
Main causes:
1) Arterial thrombo-embolic events (~75-80%)
- Primarily due to atherosclerosis
- Large vessel infractions due to:
- Artery – artery emboli
- Thrombosis in situ
- – Extra or intracranial large or medium sized vessels
- – Small vessel infractions (lacunes)
2) Cardioemboli (~20-25%)
- Atrial fibrillation (most common)
- Post myocardial infarction (MI)
- Low ejection fraction
- Mechanical valves
- Atrial myxoma
- Subacute bacterial endocarditis
3) Other important but less common causes:
- Hypoperfusion
- Focal: Due to severe arterial stenosis
- Global: Due to systemic hypoperfusion and includes
- – Myocardial infarction
- – Heart failure, poor LV function
- – Cardiac arrhythmias
- – Blood loss, severe anemia
- – Pericardial effusion
- – Medication-induced (hypotension)
- Arterial dissections
- May cause thrombo-embolic or hypoperfusion stroke or both
- Potential hypercoagulable states
- Antiphospholipid antibody syndrome
- Protein C and S deficiency
- Antithrombin III deficiency
- Factor V Leiden mutation
- JAK-2 mutation
- Other pro-coagulable conditions
- – Neoplasm
- – Peri-partum
- Peripartum sagittal sinus thrombosis/cerebral venous thrombosis (CVT) during or after pregnancy
- Increased risk of venous thromboembolic events during pregnancy and for ~6 to 8 weeks post-partum
- ~2% of pregnancy-associated strokes are attributable to CVT
- Advancing age, caesarean delivery and presence of infections, hypertension and excessive vomiting during pregnancy increases the risk of peripartum CVT
- Hematological disorders
- Thrombocytosis
- Sickle cell
- Polycythemia
- Hormone therapy/oral contraceptives
- Migraine
- Vasculitis
- Paradoxical emboli
- Compression (mass effect) on intracranial vessels
- Structural lesions (neoplasm), edema
- Infections (abscesses, basilar meningitis)
Epidemiology
Canadian:
- 15 million people suffer strokes worldwide each year. Of these, 5 million dies and another 5 million are permanently disabled
- The major cause of long-term disability in adults
- The second leading cause of death worldwide
- Third leading cause of death in Canada
- Fifth leading cause of death in the USA
- After the age of 55, risk of stroke doubles every 10 years
- Every year >50,000 Canadians and approximately 795,000 Americans suffer a stroke
- Approx: 315,000 Canadians are living with stroke or its effects
- Stroke survivor has an ~ 11% of recurrent stroke within the first year and up to ~26% recurrence at 5 years and ~39% at 10 years
- In the United States, a stroke occurs every ~40 seconds
- Stroke kills almost 140,000 Americans each year—that is 1 death ~4 minutes
Effects:
Of every 100 people who have a stroke
- 15 die (15%)
- 10 recover completely (10%)
- 25 recover with a minor impairment or disability (25%)
- 40 are left with a moderate to severe impairment (40%)
- 10 are so severely disabled they require long-term care (10%)
Economics:
- Stroke costs ~$2.8 billion /year in Canada and ~$34 billion / year in the US
Reference: Heart and Stroke Foundation of Canada; Center of disease control and prevention-2012
Pathophysiology
Risk factors for ischemic stroke:
{kind=link}
- Atherosclerosis
- Underlies most thrombo-occlusive events
- Develop within extra- or intra-cranial vessels affecting large or small vessels
- Occlusion of a small blood vessel via thrombosis in situ or from proximal emboli causes subcortical infarctions (lacunes)
- Exacerbated by age, hypertension, diabetes, smoking, hyperlipidemia
- Plaques often occur at bifurcations
- Plaque rupture triggers platelet aggregation and thrombosis in situ or distal embolization
- Putative causes of cardioembolism
- Cardioemboli lodged within cerebral vessels causes flow obstruction leading to ischemia/infarction. The composition of cardioemboli differs depending upon the cause:
{kind=link}

- Hypoperfusion – Border zone or watershed infarcts [between vascular zones e.g. middle cerebral artery (MCA) and posterior cerebral artery (PCA) or middle cerebral artery (MCA) and anterior cerebral artery (ACA) can occur from reduced cardiac output or hypotension particularly in the setting of severe stenosis]

- Paradoxical emboli
- Shunting of venous emboli into the arterial circulation most often via:
- – Patent foramen ovale
- – Atrial septal defect
- – Pulmonary fistulae (very rare)
- Dissection
- Can occur at any age but is a common cause of stroke in “young” adults <50 years of age
- May follow minor trauma
- May be associated with vascular disorders such as collagen vascular disease; fibromuscular dysplasia
- Tear may occlude vessel or narrow lumen leading to hypoperfusion or thrombo-embolic events
{kind=link}
Clinical Presentation
- Abrupt onset of persistent neurological deficit

- Clinical Features suggestive of cardioembolic cerebral infarction:
- Co-occurrence of cerebral and systemic emboli and/or stroke distributing into different vascular territories
- A Valsalva manoeuvre (straining) at the time of stroke onset may suggest paradoxical emboli
Differential Diagnosis
- Seizures with Todd’s paralysis
- Todd paralysis- transient but sometimes prolonged neuro-deficits (weakness, numbness, speech disruption) following a seizure
- Space-occupying lesion
- Neoplasm, abscess
- Migraine with aura (classic or complicated)
- Syncope – lightheaded, dizzy, unsteady, visual blurring
- Vertigo/dizziness secondary to vestibulopathy
- Radiculopathies (focal numbness/weakness)
- Neuropathies focal e.g. carpal tunnel syndrome, or diffuse numbness ± weakness
- Dementia (e.g. with speech/language impediment or dyspraxia
- Metabolic derangement
- Hypoglycemia
- Hypomagnesemia
- Conversion reaction/neuroses/stress, anxiety/malingering
- Head trauma
Investigation and Workup
History:
- Symptom presentation – rapid onset vs. stuttering course vs. gradual
- Time of onset (crucial if thrombolysis being considered)
- Collapse ±trauma at time of event (assess bleeding risk)
- Trauma just prior to event (consider arterial dissection)
- History of bleeding/ anemia
- Recent surgery
- Recent MI
- Seizure at time of event
Physical:
- Assess for airway, breathing, and circulation
- Determine BP, heart rate, oxygen saturation, and temperature
- Neurological exam/ NIHSS
- Premorbid modified Rankin scale (mRS)
{kind=link}
{kind=link}
Usual Investigations in ED:
– Blood work (all patients)
- Glucose, electrolytes, renal function tests
- Complete blood count (CBC)
- Activated partial thromboplastin time (APTT)
- Prothrombin time (PT) / International normalized ratio (INR)
- Oxygen saturation
- Cardiac biomarkers (if MI suspected)
- Type and screen (for tPA cases)
– Blood work (selected patients)
- Thrombin time (TT) and/or ecarin clotting time (ECT) if it is suspected the patient is taking direct thrombin inhibitors or direct factor Xa inhibitors
- Liver function tests
- Creatine kinase (CK) (if rhabdomyolysis suspected)
- Toxicology screen
- Blood alcohol level
- Pregnancy test
- Arterial blood gas tests (if hypoxia is suspected)
– Cardiac monitoring
- Blood pressure
- ECG/ telemetry
– Imaging
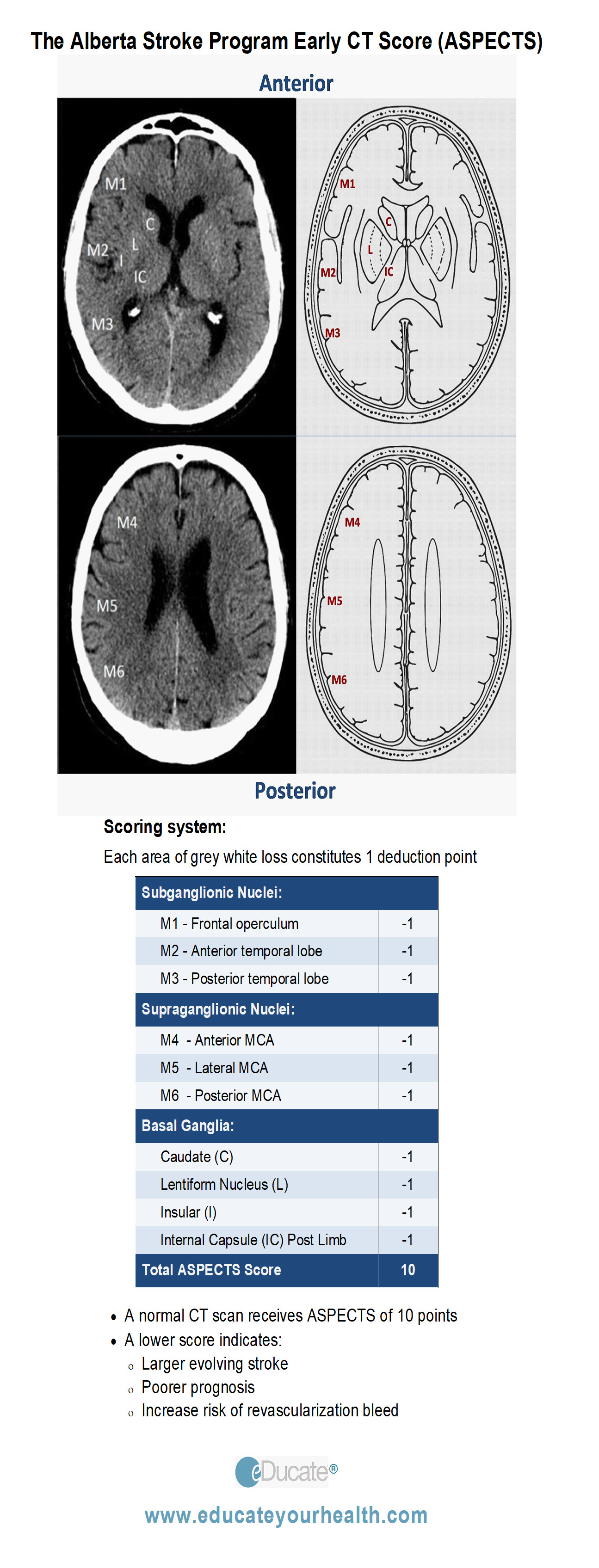
- Non-contrast CT brain (NCCT)
- The Alberta Stroke Programme Early CT Score (ASPECTS) can be useful in detecting early signs of acute ischemia
- CTA neck and head
- MRI brain with diffusion imaging (if available)
- CT and MRI perfusion studies can differentiate salvageable (the ischemic penumbra) from non-salvageable (core infarct) brain, and help identify select patients for revascularization beyond the accepted time window (up to 24hrs)
- Chest radiography (if indicated)
{kind=link}
Post ED investigations might include:
– Blood work
- CBC, glucose, electrolytes
- Partial thromboplastin time (PTT), INR
- Liver function tests (LFTs)
- Fasting cholesterol and lipid profile
- Hypercoagulable state screen (if indicated)
- Protein C and S
- Antithrombin III
- Anticardiolipin antibody
- Lupus anticoagulant
- Factor V Leiden
- JAK-2
- Vasculitis
- Antinuclear antibody (ANA)
- Rheumatoid factor (RF)
– Imaging
- Carotid and vertebral doppler ±transcarnial doppler
- Repeat CT brain ±CTA
- Diffusion MRI ±MR-angiogram (MRA)
- Chest x-ray
- Conventional (catheter) angiography
- More invasive than CTA/MRA, used less often
– Cardiovascular workup
- Holter monitor/telemetry
- Echocardiography
- Transthoracic (TTE) (commonly used, low yield)
- Transesophageal (TEE) (better visualization of anatomy, thrombus detection)
Treatment
{kind=link}
Goal:
“Is to examine and begin fibrinolytic therapy within 60 minutes of the ischemic stroke patient’s arrival in the emergency department”
General Considerations:
- Time
- Ensure hemodynamic stability plus mechanical ventilation as required
- Cardiac monitoring (assess for arrhythmia including brady- and tacy- arrhythmias as well as AF)
- Hypertension:
- Caution: Avoid overly aggressive blood pressure lowering if possible unless signs of HTN crisis/ encephalopathy or tPA use being considered
- BP up to ~220/115 mm Hg may be allowed for 24-48 hrs to encourage cerebral perfusion
- Decrease BP to <185/110 mm Hg as required for tPA administration and maintain for at least 24hr post tPA
- Intravenous fluids:
- Both hyper and hypovolemia could potentially exacerbate brain injury
- Treat hypovolemia leading to hypoperfusion
- Blood glucose:
- Treat hypo- or hyperglycemia
- Fever:
- Treat hyperthermia (acetaminophen)
- Consider septic work-up
- – Blood/ urine culture
- – Chest x-ray
- Oral intake:
- NPO until swallowing assessment to avoid aspiration
- Ins/Out:
- Avoid dehydration but avoid excess fluid and glucose infusion
- Bladder – catheterize prn to avoid bladder distension or use Foley catheter
{kind=link}
Intravenous rtPA fibrinolytic therapy:
- Thrombolysis within 4.5hr, may be complemented by direct clot retrieval via endovascular therapy (EVT)
- Intravenous rtPA (0.9 mg/kg, maximum dose 90 mg) is recommended for administration to eligible patients who can be treated in the time period of ≤4.5 hours of stroke onset
Intra-arterial rtPA fibrinolytic therapy:
- Early promising studies using IA tPA has given way to an overwhelming body of work demonstrating efficacy of endovascular therapy using retrievable stent thrombectomy devices with and without concomitant use of rtPA
Endovascular therapy (EVT):
In 2014, Berkhemer et al. presented data from a Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands (MR CLEAN) using retrievable stent thrombectomy devices to treat patient with AIS within 6 hours with or without concomitant tPA. Comparison of minor or disability at 90 days was 33% in the EVT + tPA group vs 19% with tPA only, yielding a favorable number needed to treat (NNT) of seven patients to prevent one outcome of moderate or severe disability. Importantly, there was no effect on mortality and follow-up CTA showed no residual large-vessel occlusion in 75% of the EVT + tPA group vs 33% of the tPA-only group.
Several other EVT studies in AIS have corroborated the efficacy of Intraarterial therapy +/- tPA for AIS < 6 hours, with additional extended window up to ~12 hours in select cases based on CT perfusion and multiphase CT imaging
- Interestingly, one recent non-inferiority randomized clinic trial in patients with acute ischemic stroke secondary to large-vessel occlusion (LVO) reported that the clinical functional outcome from endovascular thrombectomy alone was comparable with combined tPA within 4.5 hours + EVT, suggesting that EVT alone without tPA could be a potential option for LVO stroke (Yang et. al. NEJM, 2020)
Current recommendations for endovascular treatment in AIS:
- In conjunction with IV tPA in patients with documented large-vessel occlusion
- Solo use in patients with large vessel occlusion < 6 hours from onset but beyond the accepted 4.5-hour time window for IV tPA or those with other contraindication(s) for IV tPA use
Antiplatelet therapy:
- Aspirin: Recommended to begin within 24-48 hours following an acute non-tPA treated stroke or 24 hours after tPA was administered provided there are no bleeding complications
- The combination of aspirin and clopidogrel might be considered for initiation within 24 hours of a minor ischemic stroke or TIA and continued for 3 weeks then reverting to monotherapy
Anticoagulant:
- Heparin: No data to support use in acute stroke, however, use in select cases might be considered by a stroke specialist
- Warfarin or Direct Oral Anticoagulant Therapy: (DOAC – Dabigatran, Rivaroxaban, Apixaban, Edoxaban)
- No data to support use in acute stroke. However, may be indicated post-acute stroke care for AF-associated cardio-embolic stroke prophylaxis
DVT prophylaxis:
- Stroke patients are at high risk of DVT within the first 2 weeks. Subcutaneous administration of anticoagulants (enoxaparin 40mg preferred) is recommended for the treatment of immobilized patients to prevent DVT. Compression stockings and early mobilization are also useful
[/cq_vc_tab_item][cq_vc_tab_item tabtitle=”Medication Dose”]MEDICATIONS:
{kind=link}
Fibrin selective agents:
- ➢ Alteplase (rt-PA)
Mechanisms:
- These agents stimulate plasminogen activator à forms a complex by binding with fibrin and plasminogen
- This complex → converts residual plasminogen into plasmin, a proteolytic enzyme capable of hydrolyzing fibrin
- Unopposed plasmin digests fibrinogen and other plasma proteins, including factors V and VIII
Dose:
Acute ischemic stroke
- Intravenous rtPA 0.9 mg/kg (maximum dose 90 mg) infused over 60-minutes with 10% of the total dose administered as an initial intravenous bolus over 1 minute is recommended for administration to eligible patients who can be treated in the time period of 3 to 4.5 hours after stroke onset
{kind=link}
- ➢ Aspirin
- ➢ Clopidogrel
Mechanisms:
Aspirin
- Works through cyclooxygenase pathway (COX 1-2 )
- Inhibits platelet aggregation
- Antipyretic, anti-inflammatory and analgesic action
- Antiplatelet effects last ~7-10 days
Clopidogrel
- Binds to adenosine diphosphate (ADP) → impairs activation of receptor complex → inhibits platelet aggregation
- Antiplatelet effects last ~7-10 days
Dose:
Aspirin:
TIA and secondary prevention of atherothrombotic cerebral infarction:
- 80-325 mg daily according to the individual needs of the patient, as determined by the physician
Clopidogrel:
Recent MI/ Recent stroke/ Peripheral arterial disease (PAD)
- Oral: 75 mg PO once daily
{kind=link}
Injectable
- ➢ Heparin (unfractionated)
- ➢ Enoxaparin (LMWH)
- ➢ Dalteparin (LMWH)
- ➢ Fondaparinux
Oral anticoagulants (OAC)
- ➢ Warfarin
- ➢ Dabigatran
- ➢ Rivaroxaban
- ➢ Apixaban
- ➢ Edoxaban
Mechanism for anticoagulants:
- Inhibits thrombus formation
- May prevent propagation of existing thrombi
- No direct lytic effect on established thrombi
- Prolongs activated partial thromboplastin time (aPTT)
Dose:
{kind=link}
Prevention of venous thromboembolism (fixed-dose therapy):
- The usual prophylactic dose is 5000 units SC every 8 to 12 hours. Prophylaxis should begin on hospital admission if indicated, or 1 to 2 hours preoperatively
Note: Heparin should continue until the patient is fully ambulatory or until hospital discharge [Chest 2008;133(6 Suppl):381S-453S].
Typical use for IV heparin:
AF with concomitant TIA or minor/small ischemic stroke
- Initial IV bolus of ~60-80 IU/kg or 5000 IU
- Followed by an infusion of 12 IU/kg/hr; Max. 1000 IU/hr
- Adjusted to maintain an APTT to 1.5 – 2 times normal (usually 50 to 70 seconds)
Caveat: For patients with moderate or large strokes, the above may be modified to a low initial exposure for the avoidance of supra-therapeutic PTT and potential risk of bleeding:
- – Initial IV bolus of ~30-40 IU/kg or 2500 IU or no bolus
- – Followed by an infusion of 12 IU/kg/hr; Max. 1000 IU/hr
- – Adjusted to maintain an APTT to 1.4-1.8 times normal (suggested, but adjusted at the discretion of treating physician)
Low-molecular-weight heparins (LMWHs):
Prophylaxis of deep vein thrombosis
- Dalteparin: 5000 IU SC once daily. In clinical trials, the usual duration of administration was 12-14 days
- Enoxaparin: 40 mg (4000 IU) SC once daily. The usual duration of administration is 6-11 days
- – Dosage in renal impairment: (CrCl <30 mL/min)
- Recommended dosage is 20 mg (2000 IU) or 30 mg (3000 IU) once daily based on individual risk/benefit assessment
- Fondaparinux: 2.5 mg SC once daily if body weight ≥50 kg
- Note: Prophylactic use contraindicated in patients <50 kg.
Oral anticoagulants:
Warfarin:
Prevention/Treatment of thrombosis/embolism
- Start 2-10 mg PO once daily for 1-2 days then; adjust dose according to INR results
- Desired INR 2-3 for non-mechanical valves. Maybe acceptable for aortic bileaflet mechanical valve without thromboembolism risk factors
- OR
- INR 2.5-3.5, if concomitant mitral mechanical valve or aortic mechanical valve
Reference: Bonow Ro, Carabello BA, Chatterjee K et al. Circulation. 2008; 118: e523-e661
Dabigatran:
Prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation (NVAF)
Canada labelling:
- Age <80 year: 150 mg twice daily if creatinine clearance >30 mL/min
- Age >80 years: 110 mg twice daily if creatinine clearance >30 mL/min
- Contraindicated in creatinine clearance <30 mL/min
USA labelling:
- 150 mg PO twice daily if creatinine clearance >30 ml/min
- 75 mg PO twice daily if creatinine clearance 15-30 ml/min
Conversion from Dabigatran to parenteral anticoagulant
- Wait 12 hrs after the last dose of dabigatran before switching to a parenteral anticoagulant
Conversion from vitamin K antagonists (e.g. warfarin) to Dabigatran
- Dabigatran should only be started after vitamin K antagonists have been discontinued, and the patient’s INR found to be <2.0
Conversion from Dabigatran to vitamin K antagonists (e.g. warfarin)
- Stop dabigatran for 12 hrs then begin warfarin protocol/nomogram (see above)
Rivaroxaban:
Prevention of stroke and systemic embolism in patients with NVAF
- 20 mg PO once daily for CrCl >50 ml/min
- 15 mg PO once daily for CrCl 30-49 ml/min
Prevention of recurrent DVT and PE
- 15 mg PO twice daily for 3 weeks, followed by 20 mg once daily for CrCl >50 ml/min
- 15 mg PO twice daily for 3 weeks, followed by 20 mg once daily for CrCl 30-49 ml/min
Apixaban:
Prevention of Stroke and Systemic Embolism in Patients with NVAF
- GFR >25 ml/min: 5 mg PO twice daily
- Alternatively, 2.5 mg BID may be considered in patients with at least 2 of the following:
- Age ≥80 years
- Body weight ≤60 kg
- Serum creatinine ≥133 micromole/L (1.5 mg/dL)
Acute treatment of DVT and PE
- 10 mg BID for 7 days, followed by 5 mg BID. No dose adjustment is necessary in patients with mild or moderate renal impairment (CrCl ≥30 mL/min
Edoxaban:
Prevention of stroke and systemic embolism in patients with NVAF
- 60 mg PO once daily for CrCl >50
- 30 mg PO once daily for CrCl 30–49; low body weight ≤60 kg; or concomitant use of P-glycoprotein inhibitors (e.g. erythromycin, cyclosporine, dronedarone, quinidine, or ketoconazole, except amiodarone and verapamil
Prevention of recurrent DVT and PE
- 60 mg PO once daily for CrCl >50
- 30 mg PO once daily for CrCl 30–49; low body weight ≤60 kg; or concomitant use of P-glycoprotein inhibitors (e.g. erythromycin, cyclosporine, dronedarone, quinidine, or ketoconazole, except amiodarone and verapamil.
[/cq_vc_tab_item][/cq_vc_tabs]
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pipeline Agents
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
Core Resources:
- Andrade JG, MD, Verma A, Mitchell LB. 2018 Focused Update of the Canadian Cardiovascular Society Guidelines for the Management of Atrial Fibrillation Can J Cardiology 2018; 34: 1371-1392
- Canadian Best Practice Stroke Guidelines 2018: https://www.strokebestpractices.ca/recommendations/acute-stroke-management
- Compendium of Pharmaceuticals and Specialties (CPS). Canadian Pharmacist Association. Toronto: Webcom Inc. 2012
- Day RA, Paul P, Williams B, et al eds. Brunner & Suddarth’s Textbook of Canadian Medical-Surgical Nursing. 2nd ed. Philadelphia: Lippincott Williams and Wilkins; 2010
- Jauch EC, Saver JL, Adams HP et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. The Executive Summary is available as an online-only Data Supplement with this article at doi: 10.1161/STR.0b013e318284056a/-/DC1.
- Foster C, Mistry NF, Peddi PF, Sharma S, eds. The Washington Manual of Medical Therapeutics. 33rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2010
- Gray J, ed. Therapeutic Choices. Canadian Pharmacists Association. 6th ed. Toronto: Webcom Inc. 2011
- Katzung BG, Masters SB, Trevor AJ, eds. Basic and Clinical Pharmacology. 11th ed. New York: McGraw-Hill; 2009
- Kernan WN, Ovbiagele B, Black HR. Guidelines for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack. Stroke. 2014;45:2160-2236. doi:10.1161/STR.0000000000000024/-/DC1
- Leading Causes of Death – Males – All races and origins – United States, 2017. National Center for Chronic Disease Prevention and Health Promotion, Division for Heart Disease and Stroke Prevention. 2019 https://www.cdc.gov/healthequity/lcod/men/2017/all-races-origins/index.htm
- Longo D, Fauci A, Kasper D, et al. eds. Harrison’s Principles of Internal Medicine. 18thed. New York: McGraw-Hill; 2011
- Management of thyroid dysfunction during pregnancy and postpartum. An endocrine society clinical practice guidelines. 2007 J Clin Endocrinol Metab:92; S1-S47
- McPhee SJ, Papadakis MA, eds. Current Medical Diagnosis & Treatment. 49th ed. New York: McGraw-Hill; 2010
- Pagana KD, Pagana TJ eds. Mosby’s Diagnostic and Laboratory Test Reference. 9th ed. St. Louis: Elsevier-Mosby; 2009
- Powers WJ; Rabinstein AA, Ackerson T 2018 Guidelines for the Early Management of Patients With Acute Ischemic Stroke. A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2018;49:e46–e99. DOI: 10.1161/STR.0000000000000158
- Skidmore-Roth L, ed. Mosby’s nursing drug reference. 24th ed. St. Louis: Elsevier-Mosby; 2011
- Skidmore-Roth L. ed. Mosby’s drug guide for nurses. 9th ed. St. Louis: Elsevier-Mosby; 2011
- Stroke facts. National Center for Chronic Disease Prevention and Health Promotion, Division for Heart Disease and Stroke Prevention. 2020; https://www.cdc.gov/stroke/facts.htm
Online Pharmacological Resources:
- e-Therapeutics
- Lexicomp
- RxList
- Epocrates
- Thrombosis Canada
Journals/Clinical Trials:
- Arboix A and Alió J. Cardioembolic Stroke: Clinical Features, Specific Cardiac Disorders and Prognosis. Current Cardiology Reviews, 2010; 6: 150-161
- Appelros P, Stegmayr B and Terént A. Sex Differences in Stroke Epidemiology: A Systematic Review. Stroke. 2009;40:1082-1090. doi: 10.1161/STROKEAHA.108.540781
- Benjamin EJ, Muntner P, Alonso A. et al., Heart Disease and Stroke Statistics—2019 Update: A Report From the American Heart Association Circulation 2019; 139: 10: e56-e528
- Berkhemer OA, Fransen PS, Beumer D, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 2015;372:11–20
- Bevan S, Traylor M, Adib-Samii P et al. Genetic heritability of ischemic stroke and the contribution of previously reported candidate gene and genomewide associations. Stroke. 2012 Dec;43(12):3161-7. doi: 10.1161/STROKEAHA.112.665760. Epub 2012 Oct 4
- Campbell BCV, Mitchell PJ, Kleinig TJ, et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med. 2015;372:1009–1018
- Chisholm ME and Campbell DC. Postpartum postural headache due to superior sagittal sinus thrombosis mistaken for spontaneous intracranial hypotension. Can J Anaesth. 2001 Mar;48(3):302-4
- Connolly SJ, Eikelboom J, Joyner C et al. Apixaban in Patients with Atrial Fibrillation (AVERROES). N Engl J Med 2011; 364:806-17
- Douen AG, Pageau N and Medic S. Usefulness of Cardiovascular Investigations in Stroke Management : Clinical Relevance and Economic Implications. Stroke. 2007;38:1956-1958. doi: 10.1161/STROKEAHA.106.477760
- Douen AG, Pageau N and Medic S. Serial Electrocardiographic Assessments Significantly Improve Detection of Atrial Fibrillation 2.6-Fold in Patients With Acute Stroke. Stroke. 2008;39:480-482. doi: 10.1161/STROKEAHA.107.492595
- Edoxaban – Thrombosis Canada http://thrombosiscanada.ca/wp-content/uploads/2018/02/Edoxaban-2018Feb16.pdf
- Feigin VL, Forouzanfar MH, Krishnamurthi R, et al.; Global Burden of Diseases, Injuries, and Risk Factors Study 2010 (GBD 2010) and the GBD Stroke Experts Group. Global and regional burden of stroke during 1990-2010: findings from the Global Burden of Disease Study 2010.Lancet. 2014; 383:245–254. doi: 10.1016/S0140-6736(13)61953-4
- Fugate JE, Rabinstein AA. Absolute and Relative Contraindications to IV rt-PA for Acute Ischemic Stroke. Neurohospitalist. 2015 Jul; 5: 110–121. doi: 10.1177/1941874415578532
- Giugliano RP, Ruf CT., Braunwald E, et al. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med 2013;369:2093-2104
- Goyal M, Demchuk AM, Menon BK, et al. Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med. 2015;372(11):1019–1030
- Granger CB, Alexander JH, McMurray J J.V et al. for the ARISTOTLE Committees and Investigators. Apixaban versus Warfarin in Patients with Atrial Fibrillation. N Engl J Med 2011; 365:981-992
- Goyal M, Demchuk AM, Menon BK, et al. Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med. 2015;372(11):1019–1030
- Jickling GC, Stamova B, Ander BP et al. Prediction of cardioembolic, arterial, and lacunar causes of cryptogenic stroke by gene expression and infarct location. Stroke. 2012; 43(8):2036-41
- Kanji S, Corman C, Douen AG. Blood Pressure Management in Acute Stroke: Comparison of Current Guidelines with Prescribing Patterns
- Koositamongkol S, Sindhu S, Pinyopasakul W et al. Factors influencing functional recovery in patients with acute ischemic stroke. Collegian: The Australian Journal of Nursing Practice, Scholarship and Research (2012). Published online. doi: 10.1016/j.colegn.2012.09.002
- Kral M, Skoloudik D, Sanak D et al. Assessment of relationship between acute ischemic stroke and heart disease- protocol of a prospective observational trial. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2012 Sep; 156(3):284-289
- Mittmann N, Seung SJ, Hill MD et. al. Impact of disability status on ischemic stroke costs in Canada in the first year. Can J Neurol Sci. 2012 Nov;39(6):793-800
- Mohr JP, Albers GW, Amarenco P et al. Etiology of stroke. Stroke journal of AHA. 1997; 28: 1501-1506
- Patel MR, Mahaffey KW, Garg J, et al, for the ROCKET AF Steering Committee for the ROCKET AF Investigators. Rivaroxaban versus Warfarin in Nonvalvular Atrial Fibrillation N Engl J Med 2011; 365:883-891
- Pexman JHW, Barber PA, Hill MD. et al. Use of the Alberta Stroke Program Early CT Score (ASPECTS) for Assessing CT Scans in Patients with Acute Stroke. American Journal of Neuroradiology 2001, 22: 1534-1542
- Pexman JHW, Barber PA, Hill MD. et al. Use of the Alberta Stroke Program Early CT Score (ASPECTS) for Assessing CT Scans in Patients with Acute Stroke. American Journal of Neuroradiology 2001, 22: 1534-1542
- Pollack CV Jr, Reilly PA, van Ryn J. Idarucizumab for Dabigatran Reversal – Full Cohort Analysis. N Engl J Med. 2017;377:431-441. DOI: 10.1056/NEJMoa1707278
- Qaseem A, Chou R, Humphrey LL, et al; Clinical Guidelines Committee of the American College of Physicians. Venous thromboembolism prophylaxis in hospitalized patients: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2011;155:625–632
- Sacco RL, Diener HC, Yusuf S, Cotton D, et al; the PRoFESS Study Group. Aspirin and extended-release dipyridamole versus clopidogrel for recurrent stroke. N Engl J Med. 2008;359:1238-1251
- Saposnik G, Barinagarrementeria F, Brown RD, et al. Statement for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2011;42:1158-1192
- Saver JL, Goyal M, Bonafe A, et al. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N Engl J Med. 2015. Epub ahead of print. doi: 10.1056/NEJMoa1415061
- Siegal DM, Curnutte JT, M.D. Connolly SJ, Andexanet Alfa for the Reversal of Factor Xa Inhibitor Activity. N Engl J Med 2015; 373:2413-2424. DOI: 10.1056/NEJMoa1510991
- Tekle WG, Chaudhry SA, Fatima Z, et al. Intravenous Thrombolysis in Expanded Time Window (3-4.5 hours) in General Practice with Concurrent Availability of Endovascular Treatment. Journal of Vascular and Interventional Neurology 2012
- The ACTIVE Writing Group on behalf of the ACTIVE Investigators. Clopidogrel plus aspirin versus oral anticoagulation for atrial fibrillation in the Atrial fibrillation Clopidogrel Trial with Irbesartan for prevention of Vascular Events (ACTIVE W). The Lancet, 2006 367, Pages 1903-1912
- Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. N Engl J Med. 1995;333):1581–1587
- Weir, N.U. An update on cardioembolic stroke ( Review ) Postgraduate Medical Journal. 2008; 84(989):133-142
- Wolf PA, Abbott RD and Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke. 1991;22:983-988. doi: 10.1161/01.STR.22.8.983
- Yang P, Zhang Y, Zhang L. et.al. Endovascular Thrombectomy with or without Intravenous Alteplase in Acute Stroke. N Engl J Med. 2020, doi: 10.1056/NEJMoa200112